







In vitreoretinal surgery for the repair of rhegmatogenous retinal detachment (RRD), internal tamponade agents provide mechanical support to the retina by counteracting fluid entry through retinal breaks and stabilizing the neurosensory retina against the retinal pigment epithelium while chorioretinal adhesion develops. Contemporary tamponade selection has evolved from a simple choice between gas and silicone oil to a tailored decision based on break location (superior vs inferior), proliferative vitreoretinopathy (PVR) risk, likelihood of a second surgery, and the patient’s ability to comply with follow-up and positioning requirements.
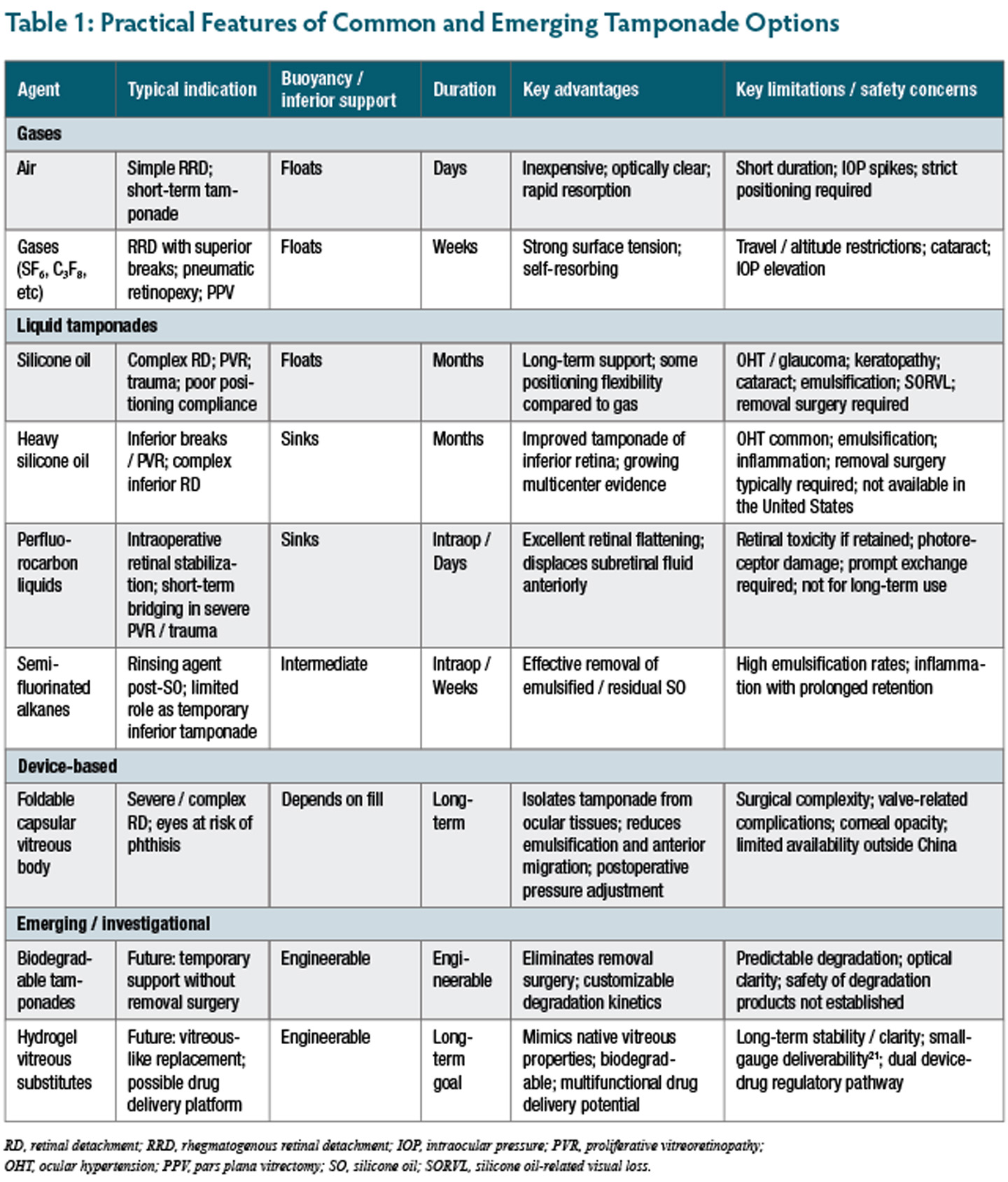
An ideal vitreous substitute would provide optical transparency, appropriate specific gravity and surface tension to prevent fluid migration, and biocompatibility without inflammation or retinal toxicity.1 Despite more than 6 decades of clinical use, currently available agents represent imperfect compromises between efficacy and safety. As a result, recent innovation has focused less on entirely novel materials and more on incremental refinements of established tamponades, improved patient selection, and strategies to mitigate complications. This review examines recent advances and emerging trends in intraocular tamponade agents (Table 1), emphasizing clinical applications, efficacy, and safety considerations.
Current Tamponade Agents
Expansile gases, such as sulfur hexafluoride (SF6) and perfluoropropane (C3F8), serve as first-line for many uncomplicated retinal detachments (RDs), particularly those with superior breaks. Hexafluoroethane (C2F6), used outside the United States, offers an intermediate duration between SF6 and C3F8 and comparable reattachment rates.2 Recent advances emphasize better patient selection, dosing discipline, and postoperative protocols—particularly travel restrictions, altitude risk, and intraocular pressure (IOP) monitoring.1 The tamponade effect is limited to days or weeks, making gas unsuitable for complex detachments requiring prolonged support.2,3
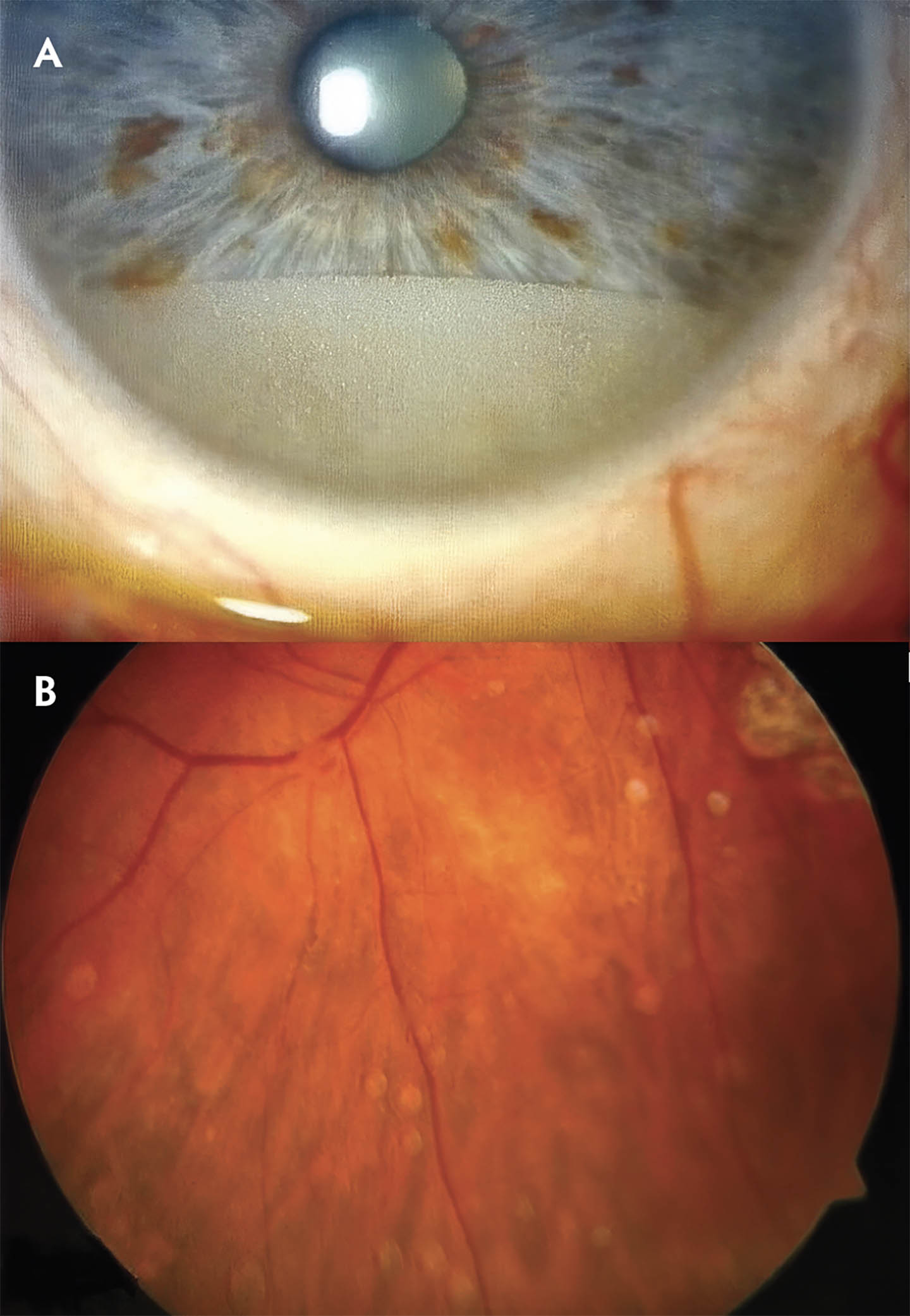
Figure 1. Heavy silicone oil emulsification. (A) Emulsified heavy silicone oil droplets in the anterior chamber. (B) Emulsified heavy silicone oil adherent to the retinal surface. From Schwarzer et al. Clinical observations and occurrence of complications following heavy silicone oil surgery. Biomed Res Int. 2014;2014:706809. doi:10.1155/2014/706809. Reproduced under CC-BY license.
Silicone oil (SO) remains essential for complex detachments, trauma, pediatric cases, and situations requiring long-term tamponade. In the management of complex PVR specifically, SO was shown to be superior to SF6 but not C3F8.4 Although SO offers some positioning flexibility compared to gas, postoperative positioning is not eliminated. Face-down or support-the-break positioning is still necessary depending on the reason the oil was placed or complexity of the break, varying from 1 to 14 days postoperatively.
Silicone oil introduces a distinct complication profile, including cataract formation, ocular hypertension or glaucoma, keratopathy, oil migration into the anterior chamber, the potential for interference with retinal imaging, and optic neuropathy in susceptible patients.5,6 An emerging concern is SO-related visual loss, an unexplained reduction in vision reported in up to 50% of macula-sparing RDs.6
Emulsification is a central limitation of SO tamponade, and there is no clear consensus on the optimal dwell time. Although most literature recommends removal at 3 to 6 months, a study using 1,000 centistoke oil found that this can be reasonably extended to 1 year with close monitoring for early signs of emulsification.7 Although 5,000-centistoke oil takes longer to emulsify, outcomes still depend on inflammation, surgical technique, and interface contaminants.5
Experimental strategies have therefore focused on altering oil composition, including the addition of high-molecular-weight polymers to increase viscoelasticity.8,9 Siluron2000 (Fluoron GmbH), a commercially available high-molecular weight silicone oil approved in Europe, has shown lower emulsification rates in clinical evaluation, though comparative trials have not demonstrated clear superiority over conventional SO.10 Recent trends emphasize complication prevention through shortening oil dwell time when feasible, aggressive control of inflammation, meticulous peripheral vitreous shaving, and close monitoring for IOP elevation and keratopathy.11
Heavy Silicone Oil
Heavy silicone oils have gained an expanded role and improved evidence base in detachments with inferior breaks and/or inferior PVR. Unlike conventional silicone oil, which floats and provides limited mechanical support to the inferior retina, heavy silicone oils such as Densiron 68 (Fluoron GmbH) and Oxane HD (Bausch + Lomb) are admixtures of high-viscosity SO and semifluorinated alkanes (SFAs) with a specific gravity greater than water.12,13 This allows them to sink and directly tamponade inferior breaks without requiring strict postoperative positioning. However, neither agent is approved for clinical use in the United States.
A proposed concern with heavy silicone oil is that superior accumulation of emulsified droplets above the main bubble may provoke a localized inflammatory response, potentially contributing to PVR formation and epiretinal membrane development. That said, clinical studies have not demonstrated a significant difference in PVR rates compared with conventional silicone oil.12,14 Moreover, recent multicenter studies and contemporary series have reported improved anatomic outcomes and postoperative visual acuity with heavy silicone oil in complex inferior RDs, with a potential retinectomy-sparing effect.12,14,15 Although these agents share many of the same risks as standard SO, including ocular hypertension, inflammation, and emulsification, their ability to address inferior pathology represents a meaningful clinical advantage in selected cases (Figure 1).6,16
Perfluorocarbon Liquids
Perfluorocarbon liquids (PFCLs) such as perfluorooctane and perfluorodecalin occupy a specialized role as intraoperative tools for retinal stabilization during vitrectomy. These heavy, optically clear fluids have nearly twice the density of water and high surface tension, allowing effective retinal flattening by displacing subretinal fluid anteriorly.6,13 In selected cases of severe PVR or ocular trauma, PFCLs have been used as short-term postoperative rescue tamponades, often in combination with silicone oil, to provide temporary inferior support while chorioretinal adhesions mature.17 Nonetheless, the risks of retinal toxicity, photoreceptor damage, and PFCL retention restrict their use to brief durations, typically no longer than 4 to 14 days. Contemporary practice emphasizes strict limitation of PFCL exposure and prompt exchange to safer long-term tamponades.17
Semifluorinated Alkanes
Semifluorinated alkanes, including perfluorobutylpentane (F4H5) and perfluorohexyloctane (F6H8), are often used intraoperatively as rinsing agents to wash residual or emulsified silicone oil from the vitreous cavity following tamponade.16 With density higher than water but lower than traditional PFCLs, SFAs could additionally be used as temporary tamponades for inferior RDs.16 Although initially promising, high emulsification rates and inflammatory complications with prolonged retention limited their clinical utility as tamponade agent. As a result, heavy silicone oils have largely replaced SFAs as the preferred option for inferior pathology.16,18
Emerging Technologies: Toward True Vitreous Substitutes
The foldable capsular vitreous body (FCVB) is a device-based approach designed to physically isolate tamponade material from intraocular tissues. The thin-walled silicone capsule is implanted through standard vitrectomy incisions and filled with balanced salt solution or SO via an integrated valve, allowing postoperative pressure adjustment.19 Clinical evaluations have reported feasibility, safety, and anatomic outcomes in severe RD settings with FCVB, with reported retinal reattachment rates ranging from 30% to 100%, depending on underlying pathology.19 By preventing direct contact between silicone oil and ocular structures, FCVB reduces complications such as anterior migration and emulsification. More recent work has explored FCVB with heavy silicone oil for complex inferior RD and PVR.20 However, inflammation, corneal opacity, and valve-related complications have been reported, and limited availability outside China has restricted widespread adoption.19
Biodegradable intraocular tamponades are designed to provide support and then degrade without requiring surgical removal. In preclinical evaluation, PYK-1105 (Pykus Therapeutics) is a hydrophilic, low-viscosity liquid injected through standard vitrectomy cannulas that rapidly cross-links in situ to form a vitreous-like gel, sealing retinal breaks by direct apposition before gradually degrading.21 However, challenges remain in achieving predictable breakdown over time, maintaining optical clarity, and ensuring that degradation products are safe for ocular tissues.21,22
Hydrogel-based vitreous substitutes represent a shift from hydrophobic tamponades toward hydrophilic biomaterials that more closely resemble native vitreous. These polymer networks offer optical transparency, viscoelastic properties similar to native vitreous, and the potential for biodegradation, eliminating the need for removal surgery.22 Achieving sufficient mechanical stability, controlled degradation rates, and reproducible manufacturing has proven challenging.
Among hyaluronic acid-based substitutes, Schulz and colleagues reported early human experience with crosslinked hyaluronic acid hydrogel in 21 phthisical eyes, demonstrating maintained IOP for a mean of 94 days (persisting up to 709 days) with preserved retinal architecture and superior biocompatibility compared to SO.23 Building on these findings, Vitargus (ABV-1701; ABCV BioPharma) represents a hyaluronic acid-based vitreous substitute that has progressed into prospective clinical evaluation (NCT04481386).22 In a phase 1 trial involving 10 patients undergoing vitrectomy for RRD or vitreous hemorrhage, the hydrogel was well tolerated, with stable retinal attachment and no reported ocular toxicity.22 Unlike silicone oil, Vitargus undergoes gradual biodegradation over several months, eliminating the need for removal surgery. Phase 2 studies are planned to further evaluate efficacy and dosing strategies.
Other hydrogel formulations with biomimetic properties have shown promise in preclinical models but have not yet been evaluated in humans. These include self-healing composite hydrogels that restore structural integrity after mechanical disruption, as well as self-assembling peptide hydrogels that achieve high optical transparency and maintain stability for several months in animal vitrectomy models without inducing retinal toxicity or inflammation.24,25 Smart hydrogel systems based on stimuli-responsive polymers offer additional advantages by responding to physiologic cues such as temperature or local chemical environment.22 Multifunctional hydrogels—including antioxidant-loaded formulations—may reduce oxidative stress or inflammation in the post-vitrectomy environment.25
Drug-Delivery Platforms
Another emerging paradigm in tamponade development recognizes that many surgical failures result not from inadequate mechanical support but from biological processes such as inflammation and PVR. As a result, there is increasing interest in tamponade agents that also function as sustained drug-delivery platforms. Silicone oil has been evaluated as a reservoir for various antiproliferative and anti-inflammatory agents, although its hydrophobic nature limits incorporation of many therapeutics.18,26
Hydrogel-based tamponades offer greater versatility for drug loading due to their hydrophilic composition. Experimental systems have demonstrated sustained release of agents such as bevacizumab over several weeks while maintaining biocompatibility.27,28 Despite promising preclinical data, drug-eluting tamponades must satisfy dual regulatory requirements as both medical devices and drug products, limiting clinical translation beyond early phase trials.
Conclusion
The contemporary landscape of intraocular tamponade is shaped by efforts to optimize existing agents and to develop materials that more closely replicate the native vitreous. There is a shift from tamponade agents acting as passive mechanical support toward novel advances involving device-based containment and drug-eluting systems. In the near term, the most meaningful gains are likely to come from evidence-guided use of heavy silicone oils in inferior pathology and from strategies to minimize complications of conventional silicone oil. Longer-term progress will depend on whether biodegradable polymers, hydrogel substitutes, and drug-eluting platforms can demonstrate the safety, durability, and clinical advantages needed to move beyond early-phase investigation. RP



REFERENCES
1. Shettigar MP, Dave VP, Chou HD, et al. Vitreous substitutes and tamponades—a review of types, applications, and future directions. Indian J Ophthalmol. 2024;72(8):1102-1111. doi:10.4103/IJO.IJO_2417_23
2. Neffendorf JE, Gupta B, Williamson TH. The role of intraocular gas tamponade in rhegmatogenous retinal detachment: a synthesis of the literature. Retina. 2018;38(suppl 1):S65-S72. doi:10.1097/IAE.0000000000002015
3. Kanclerz P, Grzybowski A. Complications associated with the use of expandable gases in vitrectomy. J Ophthalmol. 2018;2018:8606494. doi:10.1155/2018/8606494
4. Vitrectomy with silicone oil or perfluoropropane gas in eyes with severe proliferative vitreoretinopathy: results of a randomized clinical trial. Silicone Study Report 2. Arch Ophthalmol. 1992;110(6):780-792. doi:10.1001/archopht.1992.01080180052028
5. Łątkowska M, Gajdzis M, Kaczmarek R. Emulsification of silicone oils: altering factors and possible complications—a narrative review. J Clin Med. 2024;13(8):2407. doi:10.3390/jcm13082407
6. Chen Y, Kearns VR, Zhou L, et al. Silicone oil in vitreoretinal surgery: indications, complications, new developments and alternative long-term tamponade agents. Acta Ophthalmol. 2021;99(3):240-250. doi:10.1111/aos.14604
7. Toklu Y, Cakmak HB, Ergun ŞB, Yorgun MA, Simsek Ş. Time course of silicone oil emulsification. Retina. 2012;32(10):2039-2044. doi:10.1097/IAE.0b013e3182561f98
8. Caramoy A, Kearns VR, Chan YK, et al. Development of emulsification resistant heavier-than-water tamponades using high molecular weight silicone oil polymers. J Biomater Appl. 2015;30(2):212-220. doi:10.1177/0885328215575623
9. Wilson DI, Te Water Naude AD, Snead MP. Refinements in the use of silicone oil as an intraocular tamponade. Eye (Lond). 2024;38(10):1810-1815. doi:10.1038/s41433-024-03027-y
10. Arjmand P, Felfeli T, Mandelcorn ED, Mandelcorn MS. Long-term safety and efficacy of Siluron2000 with pars plana vitrectomy in the treatment of patients with severe vitreoretinopathy and chronic macular holes. Clin Ophthalmol. 2021;15:4373-4379. doi:10.2147/OPTH.S338269
11. Oliveira RAD, Magalhaes Junior O, Rossi JPDS, et al. Complications of silicone oil as vitreous tamponade in pars plana vitrectomy: a mini review. Curr Eye Res. 2025;50(4):353-361. doi:10.1080/02713683.2024.2409883
12. Tzoumas N, Yorston D, Laidlaw DAH, et al. Improved outcomes with heavy silicone oil in complex primary retinal detachment. Ophthalmology. 2024;131(6):731-740. doi:10.1016/j.ophtha.2023.12.016
13. Carlà MM, Mateo C, Giannuzzi F, Boselli F, Rizzo S. Heavy silicone oil tamponade in retinal detachment surgery: a systematic review and single-arm meta-analysis on Densiron 68 and Oxane HD. AJO Int. 2024;1(3):100055. doi:10.1016/j.ajoint.2024.100055
14. Moussa G, Tadros M, Ch’ng SW, et al. Outcomes of heavy silicone oil (Densiron) compared to silicone oil in primary rhegmatogenous retinal detachment: a multivariable regression model. Int J Retina Vitr. 2022;8(1):61. doi:10.1186/s40942-022-00413-0
15. Oliveira RAD, Pesquero VO, Ribeiro LZ, et al. Retrospective case series of high-density silicone oil (Oxane HD) in severe proliferative vitreorretinal retinal detachment patients. Int J Retina Vitr. 2024;10(1):33. doi:10.1186/s40942-024-00548-2
16. Romano MR, Ferrara M, Nepita I, et al. Biocompatibility of intraocular liquid tamponade agents: an update. Eye (Lond). 2021;35(10):2699-2713. doi:10.1038/s41433-021-01596-w
17. Pérez SMP, Arias VC, Ramírez DJ, Martínez CE, Tamayo Martínez N. Efficacy of the use of perfluorocarbon as a temporary tamponade agent in severe ocular trauma and/or complex retinopexy: a scoping review. Int J Retina Vitr. 2024;10(1):6. doi:10.1186/s40942-023-00504-6
18. Schulz A, Szurman P. Vitreous substitutes as drug release systems. Transl Vis Sci Technol. 2022;11(9):14. doi:10.1167/tvst.11.9.14
19. Abu Serhan H, Irshaidat S, Abu Serhan L, Elnahry AG. Foldable capsular vitreous body indications, complications, and outcomes: a systematic review. Graefes Arch Clin Exp Ophthalmol. 2023;261(8):2103-2116. doi:10.1007/s00417-023-05995-5
20. Lu H, Shen Y, Fan P, et al. Efficacy of foldable capsular vitreous body implants filled with light or heavy silicone oil in the treatment of silicone oil-dependent eyes. Transl Vis Sci Technol. 2024;13(9):2. doi:10.1167/tvst.13.9.2
21. Stryjewski TP, Stefater JA, Roth L, et al. PYK-1105: preclinical evaluation of a novel biodegradable vitreous substitute for retinal tamponade. J Vitreoretin Dis. 2021;5(1):32-39. doi:10.1177/2474126420946632
22. Sojdeh S, Panjipour A, Bejandi ZB, et al. Hydrogel-based vitreous substitutes. Int J Mol Sci. 2025;26(17):8406. doi:10.3390/ijms26178406
23. Schulz A, Wakili P, Januschowski K, et al. Safety and performance assessment of hyaluronic acid-based vitreous substitutes in patients with phthisis bulbi. Acta Ophthalmol. 2023;101(6):687-695. doi:10.1111/aos.15658
24. Choi G, An SH, Choi JW, et al. Injectable alginate-based in situ self-healable transparent hydrogel as a vitreous substitute with a tamponading function. Biomaterials. 2024;305:122459. doi:10.1016/j.biomaterials.2023.122459
25. Uesugi K, Sakaguchi H, Hayashida Y, et al. A self-assembling peptide gel as a vitreous substitute: a rabbit study. Invest Ophthalmol Vis Sci. 2017;58(10):4068. doi:10.1167/iovs.17-21536
26. Williams R, Cauldbeck H, Kearns V. Sustained-release drug delivery systems. Eye (Lond). 2025;39(4):658-666. doi:10.1038/s41433-024-03134-w
27. Allyn MM, Ryan AK, Rivera G, et al. In vivo assessment of an antioxidant hydrogel vitreous substitute. J Biomed Mater Res A. 2025;113(1):e37813. doi:10.1002/jbm.a.37813
28. Liu Z, Liow SS, Lai SL, et al. Retinal-detachment repair and vitreous-like-body reformation via a thermogelling polymer endotamponade. Nat Biomed Eng. 2019;3(8):598-610. doi:10.1038/s41551-019-0382-7