







Although patients with geographic atrophy (GA) secondary to age-related macular degeneration (AMD) have historically faced an inevitable course of progressive vision loss, the recent approval of therapies that slow GA growth1,2 has ushered in a new era of hope for these patients. Specifically, pivotal trials of pegcetacoplan (OAKS and DERBY)1 and avacincaptad pegol (GATHER2)2 demonstrated reductions in GA growth rates of approximately 15% over 12 months.
However, no significant treatment effect was observed for any prespecified visual function endpoints in these landmark trials—including visual acuity (VA), reading speed, and visual sensitivity on microperimetry—or patient-reported outcomes.1,2 These findings, together with observations of an increased risk of macular neovascularization1,2 and reports of retinal vasculitis associated with pegcetacoplan,3 contributed to the evidence that informed the decision of the European Medicines Agency (EMA) to reject the application for approval of pegcetacoplan. The absence of statistically significant treatment effects on prespecified visual function outcomes has also raised concerns within the clinical community regarding the appropriateness of these therapies for patients with GA.4 To help with considering the clinical value of such GA treatments, this article discusses the nature of commonly used visual function endpoints and emerging evidence from observational studies.
Fovea-Based Visual Function Endpoints in GA Trials
The ability of visual function endpoints to capture beneficial treatment effects in eyes with GA depends on 2 key characteristics:
- How well the endpoint is targeted to the nature of the disease, and
- How effectively it captures longitudinal changes, by distinguishing true disease progression from measurement variability.
Visual acuity is a commonly used functional outcome measure in GA trials,5 but it is widely recognized as limited in its ability to reflect the overall functional impact of GA.6-8 As a fovea-centered measure, VA correlates poorly with total GA area (R2=0.07), and only demonstrates a stronger association with GA involving the central 1-mm diameter region (R2=0.45).9
Reading speed shares similar limitations as a fovea-based functional measure. Longitudinal changes in reading speed show only weak correlations with changes in GA extent, further underscoring that these endpoints are not well aligned with the nature of GA progression.10
Importantly, a recent study demonstrated that measurement variability relative to detectable longitudinal change is more than 4 to 7 times higher for VA and reading speed than for objective structural measurements of GA extent.10 As a result, clinical trials powered to detect treatment effects on GA area are substantially underpowered to detect meaningful changes in VA and reading speed.
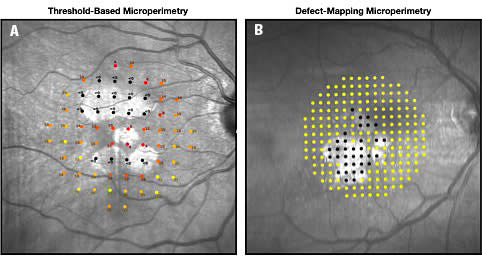
Figure 1. Comparison of (A) standard threshold-based microperimetry, which uses multiple stimulus presentations at fewer locations (68 points), and (B) novel defect-mapping microperimetry (DMP), which uses single suprathreshold stimuli presentations at a greater number of locations (208 points) in eyes with geographic atrophy. Note that DMP evaluated more than 3 times as many locations, while requiring approximately half the test duration of threshold-based microperimetry; with equivalent testing time, a DMP test would evaluate approximately 6 times as many locations.
Microperimetry: Potential and Pitfalls
Fundus-controlled perimetry, commonly referred to as microperimetry, is a technique used to assess visual sensitivity at specific retinal locations by enabling direct visualization of the fundus during testing. Conventional microperimetry involves measuring visual sensitivity thresholds, with mean sensitivity across all tested locations commonly used as an outcome measure in clinical trials.11
Threshold-based microperimetry requires repeated stimulus presentations at varying intensities. To maintain acceptable test durations, assessments can only be performed at a limited number of retinal locations. In addition, substantial measurement variability has been reported in areas of reduced visual sensitivity,12,13 which can hamper accurate characterization of visual functional loss in eyes with GA.
Given these limitations, it is not surprising that only weak correlations were observed between GA extent and both mean sensitivity and the number of absolute scotomas in the phase 3 Chroma and Spectri trials using threshold-based microperimetry (Spearman correlation coefficients, −0.45 and 0.59, respectively).14 Further analyses also showed that the level of measurement variability of these outcome measures relative to the degree of change that could be detected over time was still twice as high as seen with the structural outcome measure of GA extent.15
As a result, clinical trials powered to detect treatment effects on GA area are likely to be underpowered to demonstrate benefit using these global functional measures derived from conventional threshold-based microperimetry. Accordingly, the absence of significant treatment effects on these endpoints in recent trials should not be interpreted as evidence of no functional benefit, but they may instead reflect limitations inherent to the assessment tools used.
Optimizing the Assessment of Visual Sensitivity Loss in GA
Foundational work by Sunness and colleagues, conducted more than 30 years ago, demonstrated that areas of GA are characterized by profound visual sensitivity loss.16,17 More recent work using automated threshold-based microperimetry by Hariri and colleagues further showed that visual sensitivity declines precipitously at the GA margin.18
If visual sensitivity loss in GA is both deep and spatially localized, then a testing strategy optimized to quantify the extent of deep sensitivity loss would be expected to outperform conventional threshold-based approaches. On this basis, we previously developed a defect-mapping microperimetry (DMP) strategy that uses single stimulus presentations at a luminance corresponding to the floor of the effective dynamic range of the microperimeter.12 This approach allows assessment of a substantially larger number of retinal locations within an acceptable testing time. Figure 1 illustrates the differences between standard threshold-based microperimetry and DMP in eyes with GA.
Using this approach, we demonstrated that DMP more effectively captures progressive enlargement of deep scotomas than conventional threshold-based microperimetry.19 We subsequently showed a strong structure-function relationship between GA extent and the proportion of locations missed on DMP (Spearman correlation coefficient, 0.90),20 which was substantially stronger than that observed with threshold-based microperimetry in the Chroma and Spectri trials.14
At a pointwise level, the probability of missing a stimulus was closely related to distance from the GA margin. Locations 0 µm to 250 µm inside the GA margin were less likely to be missed than those more than 250 µm inside the margin (64% vs 88%).20 This finding is consistent with prior threshold-based microperimetry studies demonstrating residual sensitivity in the inner junctional zone.21 Conversely, locations within 0 µm to 500 µm outside the GA margin were more likely to be missed than more distal locations (>500 µm; 7% vs 2%), consistent with reduced sensitivity in the perilesional region.22 These observations align with histopathologic evidence showing that photoreceptor loss and retinal pigment epithelium dysmorphia extend beyond the clinically defined GA margin.23,24
In longitudinal analyses, we also observed moderate correlations between changes in GA extent and changes in the proportion of missed locations on DMP over 2 visits in a cohort followed at 3 monthly intervals (Spearman correlation coefficient, 0.52).25 Correlations strengthened when analyses were limited to visits separated by at least 12 months and 24 months (Spearman correlation coefficients, 0.68 and 0.87, respectively).25 By comparison, only weak correlations were observed in the Chroma and Spectri trials between longitudinal changes in GA extent and changes in mean sensitivity or number of absolute scotomas measured with standard threshold-based microperimetry over 48 weeks (Spearman correlation coefficients, approximately 0.01 and 0.26, respectively).14
Implications for Potential Benefit of Treatments
Overall, these findings based on DMP confirm the expected functional relevance of fundus autofluorescence–defined GA growth. In addition, in a recent study, we showed that customized analyses of the proportion of locations missed on DMP over time—focusing on subsets of test locations immediately adjacent to repeatably nonresponding locations at baseline—captured progressive change as effectively as the structural measure of GA extent.26
Taken together, these observations suggest that the absence of treatment benefit on prespecified visual function endpoints in pivotal trials to date may reflect limitations of the tools used to assess functional decline in eyes with GA, rather than a true absence of functional benefit.1,2 We therefore hypothesize that a randomized trial of a therapy shown to slow GA growth would likely demonstrate corresponding functional benefit when assessed with DMP. Nonetheless, it remains possible that treatment-related effects could alter the structure-function relationships observed in current observational studies, underscoring the need for confirmatory prospective evaluation.
Importantly, demonstrating treatment effects on visual function endpoints is not equivalent to demonstrating benefit in functional vision, as assessed by objective performance measures or patient-reported outcomes. In other vision-threatening diseases, such as glaucoma, performance measures including reading speed, driving risk, and wayfinding and navigation,27-30 as well as patient-reported outcomes,31,32 are associated with the severity and binocularity of visual field loss, but not always in a linear manner. In many cases, measurable impairment does not become evident until a critical threshold of binocular field loss is reached.
Measures of functional vision are inherently more variable than clinic-based visual function endpoints and often require large sample sizes and long follow-up to detect treatment effects in slowly progressive diseases. This challenge is illustrated by the United Kingdom Glaucoma Treatment study, which failed to demonstrate significant treatment benefit of latanoprost compared to placebo for generic and disease-specific patient-reported outcomes, despite clear efficacy in slowing visual field progression.33
These issues remain a central challenge in efforts to secure regulatory approval for GA therapies that slow lesion growth when clear evidence of clinically meaningful functional benefit is still difficult to demonstrate. Continued investigation into the relationship between GA and functional vision is therefore essential. In this context, recent confirmation of a strong correlation between GA extent and visual sensitivity measured with DMP provides an important foundation for future work in this area. RP


References
1. Heier JS, Lad EM, Holz FG, et al. Pegcetacoplan for the treatment of geographic atrophy secondary to age-related macular degeneration (OAKS and DERBY): two multicentre, randomised, double-masked, sham-controlled, phase 3 trials. Lancet. 2023;402(10411):1434-1448. doi:10.1016/S0140-6736(23)01520-9
2. Khanani AM, Patel SS, Staurenghi G, et al. Efficacy and safety of avacincaptad pegol in patients with geographic atrophy (GATHER2): 12-month results from a randomised, double-masked, phase 3 trial. Lancet. 2023;402(10411):1449-1458. doi:10.1016/S0140-6736(23)01583-0
3. Witkin AJ, Jaffe GJ, Srivastava SK, et al. Retinal vasculitis after intravitreal pegcetacoplan: report from the ASRS Research and Safety in Therapeutics (ReST) committee. J Vitreoretin Dis. 2023;8(1):9-20. doi:10.1177/24741264231220224
4. Spaide RF, Vavvas DG. Complement inhibition for geographic atrophy: review of salient functional outcomes and perspective. Retina. 2023;43(7):1064-1069. doi:10.1097/IAE.0000000000003796
5. Cheng QE, Gao J, Kim BJ, Ying GS. Design characteristics of geographic atrophy treatment trials: systematic review of registered trials in clinicaltrials.gov. Ophthalmol Retina. 2018;2(6):518-525. doi:10.1016/j.oret.2017.08.018
6. Sunness JS, Applegate CA, Haselwood D, Rubin GS. Fixation patterns and reading rates in eyes with central scotomas from advanced atrophic age-related macular degeneration and Stargardt disease. Ophthalmology. 1996;103(9):1458-1466. doi:10.1016/s0161-6420(96)30483-1
7. Sunness JS, Rubin GS, Applegate CA, et al. Visual function abnormalities and prognosis in eyes with age-related geographic atrophy of the macula and good visual acuity. Ophthalmology. 1997;104(10):1677-1691. doi:10.1016/s0161-6420(97)30079-7
8. Sunness JS, Rubin GS, Zuckerbrod A, Applegate CA. Foveal-sparing scotomas in advanced dry age-related macular degeneration. J Vis Impair Blind. 2008;102(10):600-610.
9. Shen LL, Sun M, Ahluwalia A, et al. Relationship of topographic distribution of geographic atrophy to visual acuity in nonexudative age-related macular degeneration. Ophthalmol Retina. 2021;5(8):761-774. doi:10.1016/j.oret.2020.11.003
10. Wu Z, Steffen V, Harris W, et al. Reading performance in geographic atrophy: comparison of different reading speed measures for capturing longitudinal changes. Ophthalmol Sci. 2024;5(3):100700. doi:10.1016/j.xops.2024.100700
11. Pfau M, Jolly JK, Wu Z, et al. Fundus-controlled perimetry (microperimetry): application as outcome measure in clinical trials. Prog Retin Eye Res. 2021;82:100907. doi:10.1016/j.preteyeres.2020.100907
12. Pfau M, Lindner M, Müller PL, et al. Effective dynamic range and retest reliability of dark-adapted two-color fundus-controlled perimetry in patients with macular diseases. Invest Ophthalmol Vis Sci. 2017;58(6):BIO158-BIO167. doi:10.1167/iovs.17-21454
13. Wu Z, Hadoux X, Jannaud M, et al. Systematic underestimation of visual sensitivity loss on microperimetry: implications for testing protocols in clinical trials. Transl Vis Sci Technol. 2023;12(7):11. doi:10.1167/tvst.12.7.11
14. Heier JS, Pieramici D, Chakravarthy U, et al. Visual function decline due to geographic atrophy: results from the Chroma and Spectri phase 3 trials. Ophthalmol Retina. 2020;4(7):673-688. doi:10.1016/j.oret.2020.01.019
15. Chang DS, Callaway NF, Steffen V, et al. Macular sensitivity endpoints in geographic atrophy: exploratory analysis of Chroma and Spectri clinical trials. Ophthalmol Sci. 2023;4(1):100351. doi:10.1016/j.xops.2023.100351
16. Sunness JS, Johnson MA, Massof RW, Marcus S. Retinal sensitivity over drusen and nondrusen areas: a study using fundus perimetry. Arch Ophthalmol. 1988;106(8):1081-1084. doi:10.1001/archopht.1988.01060140237032
17. Sunness JS, Schuchard RA, Shen N, et al. Landmark-driven fundus perimetry using the scanning laser ophthalmoscope. Invest Ophthalmol Vis Sci. 1995;36(9):1863-1874.
18. Hariri AH, Tepelus TC, Akil H, et al. Retinal sensitivity at the junctional zone of eyes with geographic atrophy due to age-related macular degeneration. Am J Ophthalmol. 2016;168:122-128. doi:10.1016/j.ajo.2016.05.007
19. Wu Z, Cimetta R, Caruso E, Guymer RH. Performance of a defect-mapping microperimetry approach for characterizing progressive changes in deep scotomas. Transl Vis Sci Technol. 2019;8(4):16. doi:10.1167/tvst.8.4.16
20. Wu Z, Hadoux X, Jannaud M, et al. Visual sensitivity loss in geographic atrophy: structure-function evaluation using defect-mapping microperimetry. Invest Ophthalmol Vis Sci. 2024;65(1):36.
21. Pfau M, von der Emde L, Dysli C, et al. Light sensitivity within areas of geographic atrophy secondary to age-related macular degeneration. Invest Ophthalmol Vis Sci. 2019;60(12):3992-4001.
22. Pfau M, Müller PL, von der Emde L, et al. Mesopic and dark-adapted two-color fundus-controlled perimetry in geographic atrophy secondary to age-related macular degeneration. Retina. 2020;40(1):169-180. doi:10.1097/IAE.0000000000002337
23. Zanzottera EC, Ach T, Huisingh C, et al. Visualizing retinal pigment epithelium phenotypes in the transition to atrophy in neovascular age-related macular degeneration. Retina. 2016;36 Suppl 1(Suppl 1):S26-S39. doi:10.1097/IAE.0000000000001330
24. Sarks J, Sarks S, Killingsworth M. Evolution of geographic atrophy of the retinal pigment epithelium. Eye (Lond). 1988;2 (Pt 5):552-577. doi:10.1038/eye.1988.106
25. Saeed A, Guymer RH, Hadoux X, et al. Longitudinal changes of visual sensitivity with geographic atrophy progression assessed by defect-mapping microperimetry. Invest Ophthalmol Vis Sci. 2024;65(14):13.
26. Saeed A, Guymer RH, Hadoux X, et al. Customized evaluation of progressive visual sensitivity loss in geographic atrophy to improve the power of clinical trials. Ophthalmol Sci. 2025;5(4):100763. doi:10.1016/j.xops.2025.100763
27. Diniz-Filho A, Boer ER, Elhosseiny A, et al. Glaucoma and driving risk under simulated fog conditions. Transl Vis Sci Technol. 2016;5(6):15. doi:10.1167/tvst.5.6.15
28. Daga FB, Macagno E, Stevenson C, et al. Wayfinding and glaucoma: a virtual reality experiment. Invest Ophthalmol Vis Sci. 2017;58(9):3343-3349.
29. Lam AKN, To E, Weinreb RN, et al. Use of virtual reality simulation to identify vision-related disability in patients with glaucoma. JAMA Ophthalmol. 2020;138(5):490-498. doi:10.1001/jamaophthalmol.2020.0392
30. Ramulu PY, West SK, Munoz B, et al. Glaucoma and reading speed: the Salisbury Eye Evaluation Project. Arch Ophthalmol. 2009;127(1):82-87. doi:10.1001/archophthalmol.2008.523
31. Abe RY, Diniz-Filho A, Costa VP, et al. The impact of location of progressive visual field loss on longitudinal changes in quality of life of patients with glaucoma. Ophthalmology. 2016;123(3):552-557. doi:10.1016/j.ophtha.2015.10.046
32. Daga FB, Gracitelli CPB, Diniz-Filho A, Medeiros FA. Is vision-related quality of life impaired in patients with preperimetric glaucoma? Br J Ophthalmol. 2019;103(7):955-959. doi:10.1136/bjophthalmol-2018-312357
33. Jones L, Garway-Heath DF, Azuara-Blanco A, et al. Are patient self-reported outcome measures sensitive enough to be used as endpoints in clinical trials?: evidence from the United Kingdom Glaucoma Treatment Study. Ophthalmology. 2019;126(5):682-689. doi:10.1016/j.ophtha.2018.09.034