







Endogenous endophthalmitis, which occurs through hematogenous dissemination of an infectious nidus to the choroid, accounts for approximately 5% to 10% of all endophthalmitis cases. Fungal and bacterial organisms each account for roughly half of these cases. Numerous risk factors have been identified, with malignancy, intravenous drug use, and immunosuppression being the primary risk factors for endogenous fungal endophthalmitis (EFE).
As an inherently systemic disease, endogenous endophthalmitis requires systemic therapy. Explicit guidelines for managing EFE are limited and largely based on low-quality evidence. The 2016 Infectious Diseases Society of America guidelines for endogenous Candida endophthalmitis recommend systemic fluconazole or voriconazole for all patients, with adjunctive intravitreal antifungals for eyes with macular involvement or vitritis, and vitrectomy considered only in severe cases for vitreous debulking.1 Notably, no guidelines exist regarding the optimal route of systemic therapy.
Historically, amphotericin B was the primary systemic agent used for management of EFE. Newer antifungal classes, including echinocandins (eg, micafungin, caspofungin) and triazoles (eg, fluconazole, voriconazole), have fewer adverse effects. Amphotericin B and echinocandins exhibit poor intraocular penetration, whereas fluconazole and voriconazole penetrate the eye effectively and are now preferred for most patients.
Oral fluconazole and voriconazole achieve at least 90% bioavailability in healthy patients, suggesting that oral and intravenous (IV) administration should have equivalent efficacy.2,3 Intraocular studies in healthy patients demonstrate adequate therapeutic aqueous and vitreous concentrations with oral administration.4,5 However, studies in patients with invasive fungal infections indicate that higher oral voriconazole doses may be required to achieve therapeutic blood concentrations.6 In both healthy and infected populations, an IV loading dose of voriconazole achieves steady-state concentrations more rapidly. To date, no studies have evaluated intraocular penetration of oral or IV fluconazole or voriconazole in inflamed or infected eyes.
Few studies have specifically addressed treatment strategies in EFE. A 2012 study described management of 65 eyes in 51 patients, noting that combination systemic and intravitreal therapy was used in only 43% of eyes.7 One-quarter of patients received systemic amphotericin B, and nearly all eyes underwent pars plana vitrectomy (PPV). Oral fluconazole was the most used systemic agent, and amphotericin B was the most frequently administered intravitreal agent.
Study Details
We initially conducted a single- institution study to evaluate factors associated with the choice of oral vs IV systemic therapy.8 Systemic culture positivity was the only factor associated with higher likelihood of IV antifungal initiation. Eyes initially treated with oral antifungals were more likely to undergo PPV than those started on IV therapy, though this difference did not reach statistical significance. Evidence of vision-threatening disease, such as vitritis or macular chorioretinitis, did not influence the initial systemic therapy route.
To increase statistical power and explore systemic treatment strategies and outcomes more comprehensively, we expanded the study to include 8 academic institutions across the United States. Investigators collected demographic, clinical, treatment, and outcome data on patients with culture-proven or clinically diagnosed EFE using electronic health records from 2010 to 2025. The primary goal was to compare outcomes based on clinical characteristics, treatment strategies, and geographic region.
Major Findings
A total of 118 eyes from 87 patients met inclusion criteria. Candida was the most frequently identified organism, while mold and culture-negative cases each accounted for approximately 20% of patients. In contrast to the 2012 study, 72% of eyes received combination systemic and intravitreal antifungals. Consistent with our single-institution study, patients with positive systemic cultures were more likely to receive IV antifungals, whereas patients with positive intraocular fluid cultures were more likely to receive oral antifungals initially.
Voriconazole (34%) and fluconazole (30%) were the most frequently used initial systemic agents. Oral fluconazole was used in 62% of cases, and IV voriconazole in 53%. Among eyes receiving intravitreal antifungals, 65% received voriconazole initially, 35% received amphotericin B, and 14% received both agents at some point during therapy.
Overall, only 30% of eyes underwent surgical intervention. Eyes initially treated with oral therapy were more likely to undergo surgery than those treated with IV therapy. Neither the route of systemic therapy nor surgical intervention affected visual acuity outcomes.
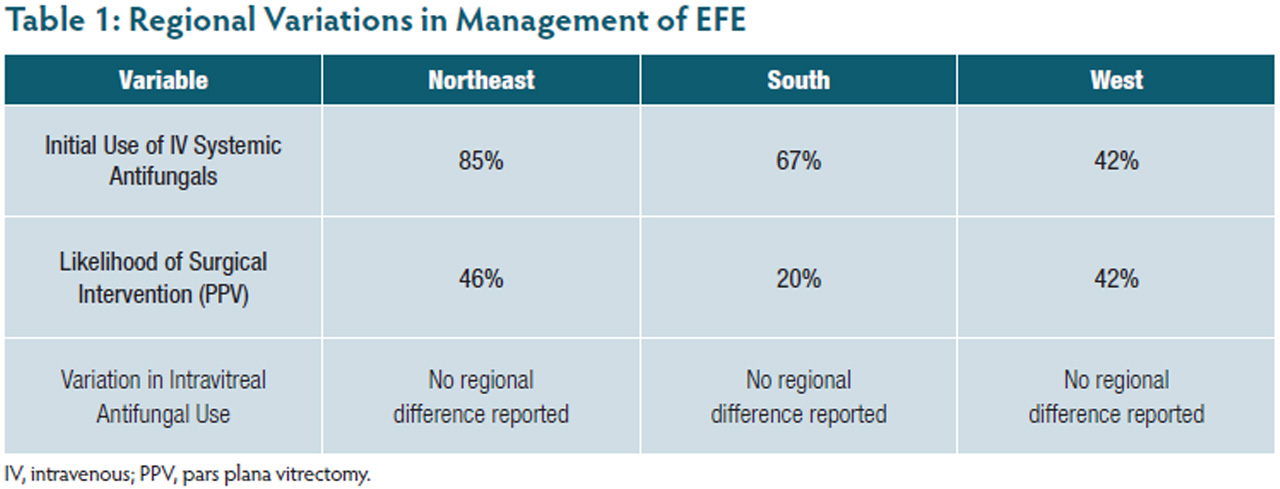
Regional practice patterns varied (Table 1). In the Northeast, 85% of patients were started on IV systemic therapy, compared with 67% in the South and 42% in the West. Northeastern eyes were also more likely to undergo surgery (46%) than eyes in the South (20%) and West (37%). No regional differences were observed in intravitreal therapy use.
Conclusion
Management of endogenous fungal endophthalmitis is complex, with wide variation in treatment strategies. Systemic markers of disease appear to influence the choice of initial therapy more than ocular findings. Although no definitive evidence favors IV over oral systemic therapy, a comprehensive, multidisciplinary approach that considers ocular involvement is essential to optimize patient outcomes in EFE. RP


References
1. Pappas PG, Kauffman CA, Andes DR, et al. Clinical practice guideline for the management of candidiasis: 2016 update by the Infectious Diseases Society of America. Clin Infect Dis. 2016;62(4):e1-e50. doi:10.1093/cid/civ933
2. Brammer KW, Farrow PR, Faulkner JK. Pharmacokinetics and tissue penetration of fluconazole in humans. Rev Infect Dis. 1990;12 Suppl 3:S318-S326. doi:10.1093/clinids/12.supplement_3.s318
3. Johnson LB, Kauffman CA. Voriconazole: a new triazole antifungal agent. Clin Infect Dis. 2003;36(5):630-637. doi:10.1086/367933
4. Aust R, Kruse FE, Wildfeuer A, Pfaff G, Rohrschneider K, Völcker HE. Fluconazole level in aqueous humor after oral drug administration in humans. Article in German. Ophthalmologe. 1995;92(6):829-832.
5. Hariprasad SM, Mieler WF, Holz ER, et al. Determination of vitreous, aqueous, and plasma concentration of orally administered voriconazole in humans. Arch Ophthalmol. 2004;122(1):42-47. doi:10.1001/archopht.122.1.42
6. Veringa A, Geling S, Span LF, et al. Bioavailability of voriconazole in hospitalised patients. Int J Antimicrob Agents. 2017;49(2):243-246. doi:10.1016/j.ijantimicag.2016.10.010
7. Chen KJ, Wu WC, Sun MH, Lai CC, Chao AN. Endogenous fungal endophthalmitis: causative organisms, management strategies, and visual acuity outcomes. Am J Ophthalmol. 2012;154(1):213-214. doi:10.1016/j.ajo.2012.03.016
8. Burton E, Reddy V, Venkat AG. Endogenous fungal endophthalmitis: a single-center retrospective study and review of the literature. Am J Ophthalmol. 2024;262:97-106. doi:10.1016/j.ajo.2024.01.018