







Optical coherence tomography (OCT) represents a significant advancement in ophthalmic imaging, enabling in vivo imaging of the retina, optic nerve, anterior segment, and other structures within the eye. Essentially, OCT uses low-coherence interferometry to establish differences in depth of tissue being imaged. This was first used to capture retinal images in vivo in 1991 by Huang et al.1 Early OCT systems employed time-domain (TD) technology, which later evolved into spectral-domain (SD) and swept-source (SS) OCT. These advanced modalities use broad-bandwidth and narrow-bandwidth light sources, respectively, to achieve faster acquisition and improved image resolution.2,3 The commercialization of OCT over recent decades has transformed ophthalmic imaging, leading to the widespread adoption of systems developed by various manufacturers. Ongoing technological progress, including the advent of OCT angiography (OCTA), continues to refine its role in clinical practice.
OCTA has emerged as an essential modality in modern retinal imaging. By detecting motion contrast from the reflectivity of moving red blood cells and analyzing decorrelation signals between sequential B-scans, OCTA visualizes vascular networks across ocular layers, with the retinal and choroidal circulations being the most extensively studied.4 This method relies on the principle that only circulating red blood cells within the retinal vasculature are moving in the retina. This technology enables the generation of depth-resolved angiograms without the need for intravenous fluorescein or indocyanine green dye, allowing clear differentiation between the different layers of the retina, including the retinal and choroidal circulations. By eliminating the need for dye injection, OCTA offers a faster, noninvasive alternative for evaluating retinal vascular diseases. In this article, we discuss the practical applications of OCTA in the modern retina clinic, as well as the advantages and disadvantages in comparison to other imaging modalities and workflow considerations in practice.
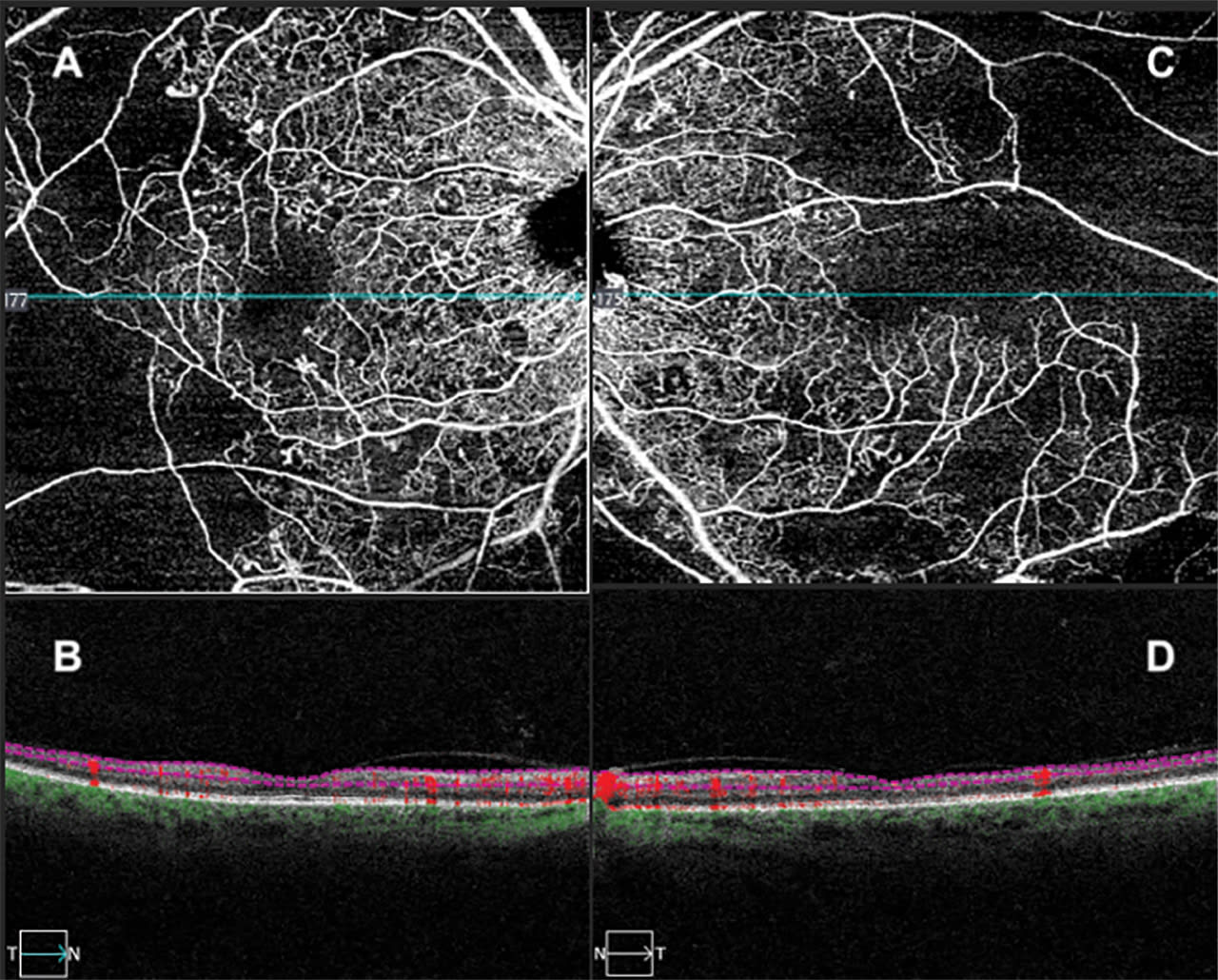
Figure 1. In a 55-year-old male with diabetic retinopathy, swept-source optical coherence tomography angiography 6x6 mm scans show an enlarged, irregular foveal avascular zone demonstrating ischemic maculopathy as well as profound capillary dropout in the superficial plexus of the right eye (A, B) and left eye (C, D).
Integrating OCTA in the Retina Clinic
OCTA can be used to evaluate a wide variety of ophthalmic conditions that affect the retinal vasculature, choriocapillaris, and choroid. These include non-neovascular and neovascular age-related macular degeneration (AMD), diabetic retinopathy, retinal vein occlusions, central serous chorioretinopathy (CSCR), macular telangiectasia, and choroidal neovascularization (CNV) due to other retinal diseases such as myopic degeneration. For AMD, OCTA can be used to visualize areas of macular neovascularization (MNV) at different segmentations.5,6 When evaluating diabetic retinopathy, OCTA offers the ability to assess for microaneurysms, neovascularization, areas of retinal nonperfusion, and changes to the foveal avascular zone.7 Furthermore, the advent of widefield OCTA, similar to widefield fluorescein angiography (FA), has been shown to have comparable results in the detection of peripheral retinal nonperfusion and areas of neovascularization.8,9 In addition, OCTA can be used to evaluate areas of capillary nonperfusion in conditions such as branch retinal vein occlusions (BRVO), central retinal vein occlusions (CRVO), branch retinal artery occlusions (BRAO), and central retinal artery occlusions (CRAO).5 Overall, OCTA serves as a valuable noninvasive modality for assessing common retinal diseases in the clinical setting.
Clinical Advantages and Limitations
OCTA is noninvasive, eliminating the need for the intravenous access and dye injection required in FA and indocyanine green angiography (ICGA). This feature decreases clinic time and patient discomfort while eliminating the risk of adverse reactions associated with dye-based procedures, such as urticaria, syncope, nausea, vomiting, and, in rare cases, anaphylaxis. The Fluorescein Angiography Complication Survey (FACS) reported a death-risk rate of 1 in 222,000, representing a non-zero risk of severe adverse events in angiographic studies.10
Inherently, OCTA does not pose such risks to patients; the only requirement in OCTA is patient fixation and compliance. Furthermore, widefield OCTA was found to be more comfortable for patients in comparison to FA, suggesting that OCTA is more tolerable in actual practice.10 FA and ICGA not only require the injection of their respective dyes, but also a dedicated technician who has proper training in both the insertion of intravenous catheters and the technicalities of photography. This requires additional manpower and time compared to OCTA, which can be performed by a standard ophthalmic technician and requires minimal training. Due to these advantages, OCTA can be a great addition to a standard retina practice and save time and expenses.
Limitations to OCTA include that its reliance on patient fixation and cooperation can lead to motion artifact, the most encountered issue. In addition, media opacities, segmentation errors, and signal attenuation can reduce image quality and interpretability, highlighting the importance of careful acquisition and review.11,12 However, having an experienced technician taking the images and providing appropriate patient education can remove many of these artifacts. Moreover, as with other imaging modalities, complete artifact removal is not required for accurate interpretation of OCTA images.
Other limitations of OCTA include the inability to assess for hyperpermeability and the breakdown of the blood-retinal barrier, as well as lesions that have slow flow. Although OCTA offers detailed, depth-resolved visualization of retinal perfusion, it lacks the ability to assess vascular hyperpermeability and delineates vasculature solely through flow-based signals. Conversely, FA reveals leakage patterns indicative of hyperpermeability. This is mainly essential for inflammatory conditions that cause posterior uveitis and retinal vasculitis.7 Although recent developments in OCTA algorithms for leakage detection are encouraging, FA continues to serve as the clinical gold standard for evaluating vascular leakage.13
Workflow Considerations
Given its speed and noninvasive nature, OCTA is a beneficial addition in a standard retina practice in the right clinical setting. Most standard commercial OCT platforms have integrated OCTA capabilities and usually takes about the same amount of time to obtain a standard OCT. In practice, it would be imperative to train ophthalmic technicians in OCTA operations, because setup (ie, patient alignment and fixation) has a crucial role in conjunction with interpretation. Furthermore, training technicians to recognize artifacts is essential to ensure optimal image acquisition and enhance the accuracy of image interpretation.
Given that OCTA is a newer technology in the retina specialist’s diagnostic arsenal, it is essential for the provider to learn how to properly interpret OCTA images. For example, understanding the disease process in conditions like AMD and diabetic retinopathy will allow clear communication between the imaging technician in terms of scan selection (ie, 3x3 mm, 6x6 mm, 12x12 mm). The provider should complete a layer-by-layer review of the superficial capillary plexus, deep capillary plexus, and choriocapillaris to ensure that no pathology is missed on a cursory glance. However, knowing how to adjust the segmentations lines to isolate the area of interest and potentially fix segmentation errors on the OCTA machine can streamline the process and lead to the right diagnosis.
Conclusion
OCTA is a valuable imaging modality that offers a rapid and safe alternative to FA and ICGA. It carries minimal risk of adverse events, and reduced personnel requirements enhance clinical efficiency and workflow. Although limitations including image artifacts and reduced sensitivity for detecting vascular hyperpermeability may temper its adoption, the low-risk profile and speed of OCTA make it a practical and complementary tool in modern retina practice for the evaluation of retinal pathologies. RP




References
1. Huang D, Swanson EA, Lin CP, et al. Optical coherence tomography. Science. 1991;254(5035):1178-1181. doi:10.1126/science.1957169
2. Wojtkowski M, Leitgeb R, Kowalczyk A, Bajraszewski T, Fercher AF. In vivo human retinal imaging by Fourier domain optical coherence tomography. J Biomed Opt. 2002;7(3):457-463. doi:10.1117/1.1482379
3. Choma MA, Hsu K, Izatt JA. Swept source optical coherence tomography using an all-fiber 1300-nm ring laser source. J Biomed Opt. 2005;10(4):44009. doi:10.1117/1.1961474
4. Kim DY, Fingler J, Zawadzki RJ, et al. Optical imaging of the chorioretinal vasculature in the living human eye. Proc Natl Acad Sci U S A. 2013;110(35):14354-14359. doi:10.1073/pnas.1307315110
5. de Carlo TE, Romano A, Waheed NK, Duker JS. A review of optical coherence tomography angiography (OCTA). Int J Retina Vitreous. 2015;1:5. doi:10.1186/s40942-015-0005-8
6. Jia Y, Bailey ST, Wilson DJ, et al. Quantitative optical coherence tomography angiography of choroidal neovascularization in age-related macular degeneration. Ophthalmology. 2014;121(7):1435-1444. doi:10.1016/j.ophtha.2014.01.034
7. Chua J, Sim R, Tan B, et al. Optical coherence tomography angiography in diabetes and diabetic retinopathy. J Clin Med. 2020;9(6):1723. doi:10.3390/jcm9061723
8. Hirano T, Kakihara S, Toriyama Y, Nittala MG, Murata T, Sadda S. Wide-field en face swept-source optical coherence tomography angiography using extended field imaging in diabetic retinopathy. Br J Ophthalmol. 2018;102(9):1199-1203. doi:10.1136/bjophthalmol-2017-311358
9. Sawada O, Ichiyama Y, Obata S, et al. Comparison between wide-angle OCT angiography and ultra-wide field fluorescein angiography for detecting non-perfusion areas and retinal neovascularization in eyes with diabetic retinopathy. Graefes Arch Clin Exp Ophthalmol. 2018;256(7):1275-1280. doi:10.1007/s00417-018-3992-y
10. Yannuzzi LA, Rohrer KT, Tindel LJ, et al. Fluorescein angiography complication survey. Ophthalmology. 1986;93(5):611-617. doi:10.1016/s0161-6420(86)33697-2
11. Holmen IC, Konda SM, Pak JW, et al. Prevalence and severity of artifacts in optical coherence tomographic angiograms. JAMA Ophthalmol. 2020;138(2):119-126. doi:10.1001/jamaophthalmol.2019.4971
12. Anvari P, Ashrafkhorasani M, Habibi A, Falavarjani KG. Artifacts in optical coherence tomography angiography. J Ophthalmic Vis Res. 2021;16(2):271-286. doi:10.18502/jovr.v16i2.9091
13. Farinha C, Santos T, Marques IP, et al. OCT-leakage mapping: a new automated method of oct data analysis to identify and locate abnormal fluid in retinal edema. Ophthalmol Retina. 2017;1(6):486-496. doi:10.1016/j.oret.2017.03.004