







Surgeons managing proliferative vitreoretinopathy (PVR) may soon have stronger evidence to support adjunctive intravitreal methotrexate, according to results presented at the 2025 American Academy of Ophthalmology (AAO) meeting. In the phase 3 GUARD clinical trial, eyes treated with intravitreal methotrexate 0.8% (ADX-2191; Aldeyra Therapeutics) experienced fewer postoperative complications, including lower rates of hypotony and cystoid macular edema (CME), compared with historical controls.
Christina J. Flaxel, MD, of the Casey Eye Institute at Oregon Health and Science University (OHSU) in Portland, a GUARD investigator, presented the data during Retina Subspecialty Day in Orlando, Florida. Disclosing that Aldeyra had provided a research grant to OHSU, she described the trial design, outcomes, and safety profile for this investigational formulation of methotrexate used during PVR repair.
ADX-2191 is a proprietary, vitreous-compatible formulation of methotrexate designed for intravitreal injection. Compared with compounded methotrexate, ADX-2191 delivers the same 400 µg dose in half the typical volume (0.05 mL). “This smaller volume is much better when you’re injecting an eye under pressure,” noted Dr. Flaxel. ADX-2191 also offers a 2-year shelf life, balanced pH and osmolarity, and optimized density that allows it to sink in oil, she said.
In the GUARD trial, which was completed in 2022, eligible eyes included those with recurrent retinal detachments due to PVR and at least 3 clock hours of star folds or epiretinal membranes, or open-globe injury with associated detachment. The original plan randomized patients to surgical repair plus ADX-2191 vs surgery alone. However, reluctance by some investigators to withhold any methotrexate led to low enrollment in the control arm, explained Dr. Flaxel.
To address this, the primary endpoint was revised to compare the treated cohort against historical controls drawn from prior PVR trials. Participants received 13 injections over 4 months—1 intraoperative dose, then weekly for 8 weeks, followed by biweekly administration for 4 weeks.
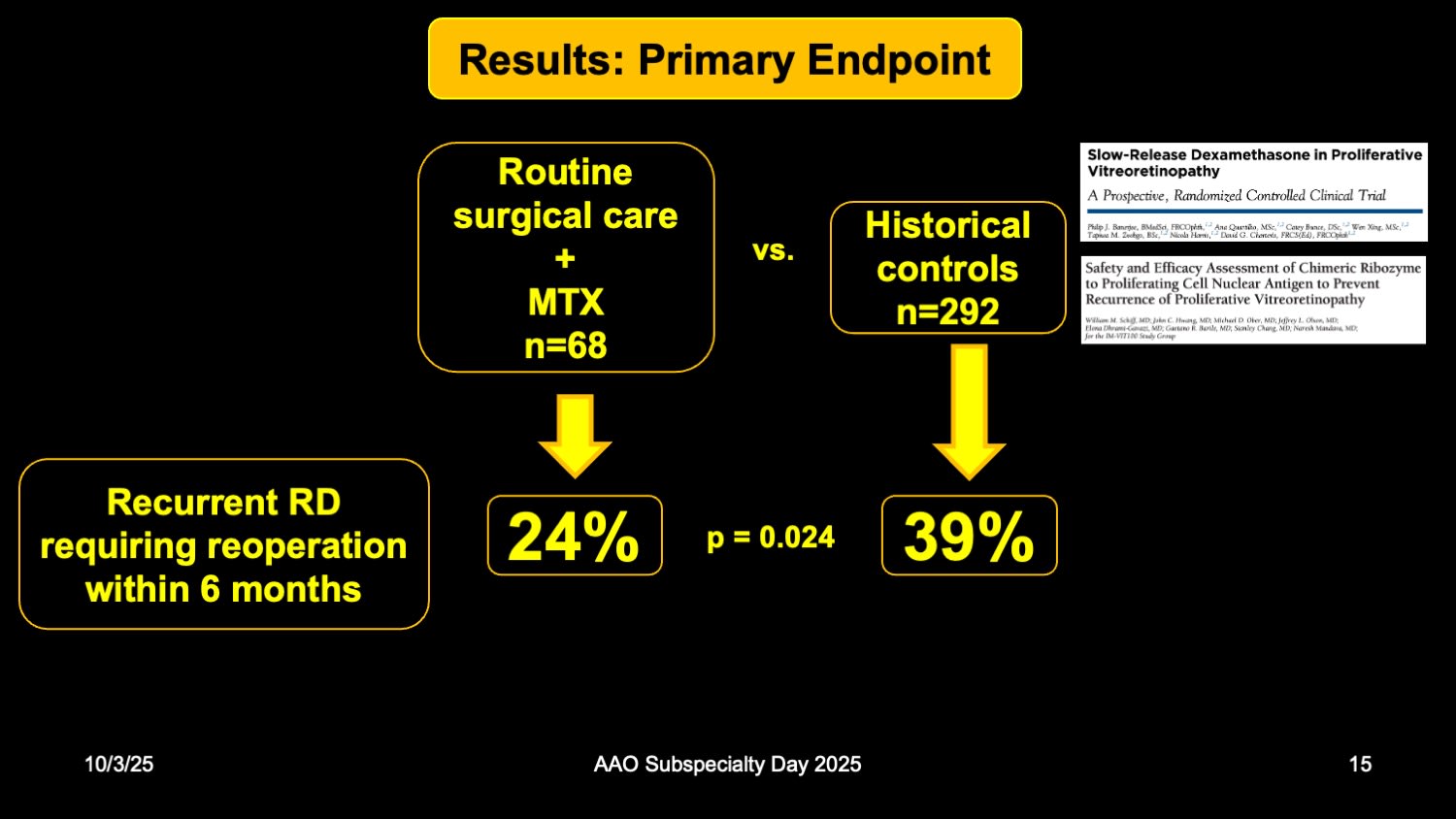
Using historical controls, the investigators reported a 24% 6-month reoperation rate in the ADX-2191 group compared with 39% in controls (P=.024). “There’s fewer retinal detachments in the methotrexate group, fewer cases of hypotony, and fewer cases of macular edema,” Dr. Flaxel noted (Figure 1). The most common adverse event associated with ADX-2191 was mild to moderate punctate keratitis, which occurred in 11 cases (16%). Previous studies using compounded methotrexate had reported rates of punctate keratitis up to 58%.
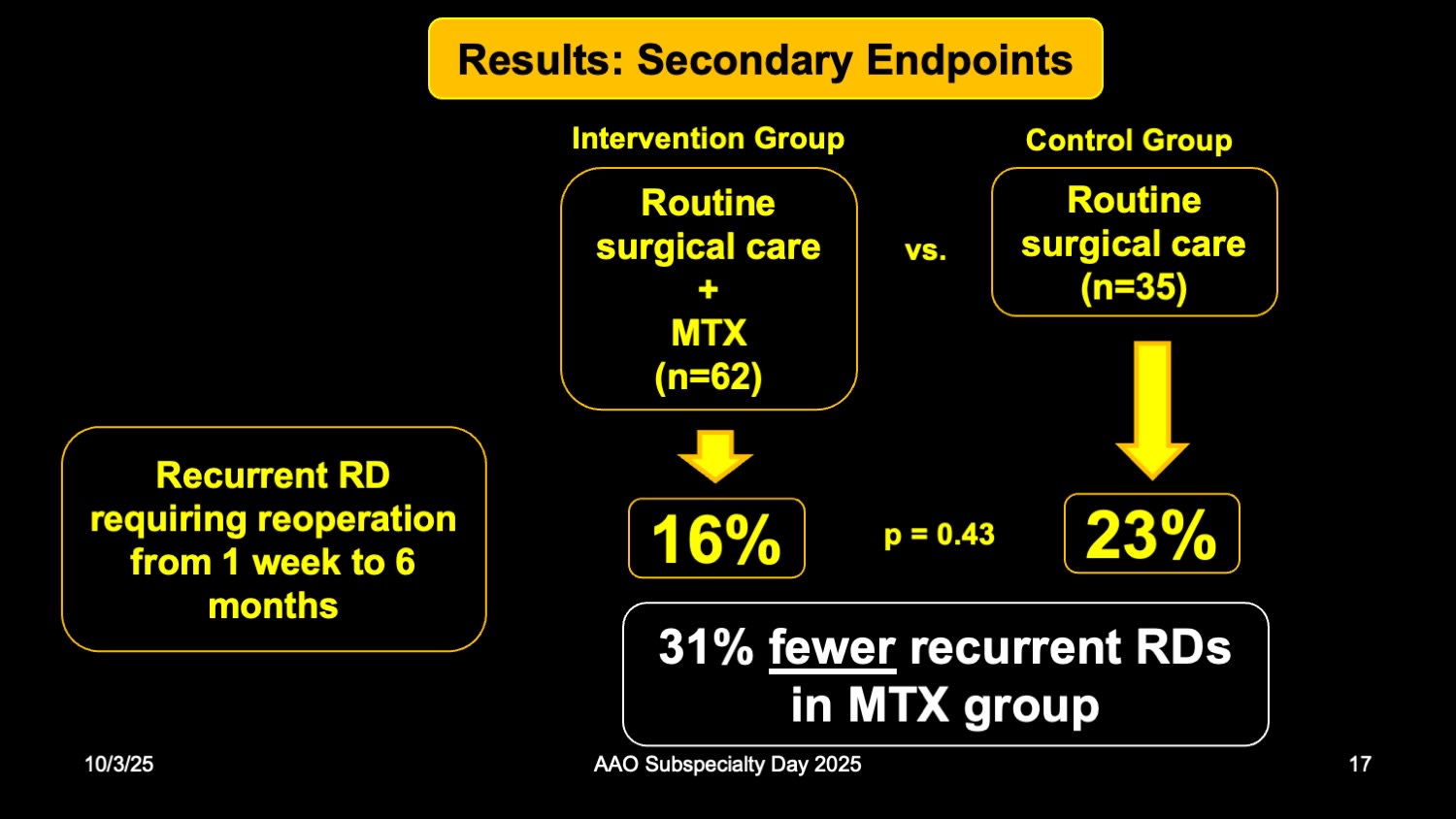
Figure 2. Six-month reoperation rates by treatment group in the GUARD trial. Among patients randomized to surgery plus ADX-2191 versus surgery alone, reoperation was required in 16% and 23% of eyes, respectively—a 31% relative reduction that did not reach statistical significance.
Among 68 patients in the methotrexate arm and 38 in the surgical-only arm, reoperation rates were 16% and 23%, respectively (P=.43). “The study was underpowered to detect a difference,” said Dr. Flaxel. “However, even though this wasn’t statistically significant, that was still 31% fewer detachments in the methotrexate group (Figure 2).” She emphasized that hypotony was significantly less common in the ADX-2191 group, and CME also occurred less frequently—an effect that has been seen in other studies presenting the off-label use of methotrexate.1,2
“Routine surgical care plus ADX-2191 was numerically superior to routine surgical care for all prespecified continuous and dichotomous endpoints, with fewer post-operative adverse events occurring following ADX-2191,” concluded Dr. Flaxel. RP
References
1. Liu T, Runer M, Mahmoud TH, et al. A modified intravitreal methotrexate protocol for the prevention of proliferative vitreoretinopathy after silicone oil removal. Ophthalmol Retina. 2025;9(4):314-321. doi:10.1016/j.oret.2024.10.006
2. Ullah A, Toth CA, Burnett HW, et al. Low-dose intravitreal methotrexate for proliferative vitreoretinopathy. Ophthalmic Surg Lasers Imaging Retina. 2023;54(3):139-146. doi:10.3928/23258160-20230220-01