







Geographic atrophy (GA), an advanced form of dry age-related macular degeneration (AMD), presents unique challenges for patient management within a retinal care setting.1,2 The FDA's approval of pegcetacoplan (Syfovre, Apellis) and avacincaptad pegol (Izervay, Astellas) for GA treatment in 2023 introduced new considerations in office dynamics and patient care protocols.3,4 As retinal specialists, adapting our practices to effectively manage and treat the increasing number of GA patients using these novel therapies is crucial. Here, we will explore best practices for patient identification, education, and support, as well as treatment decisions and resource management.
Patient Identification and Education
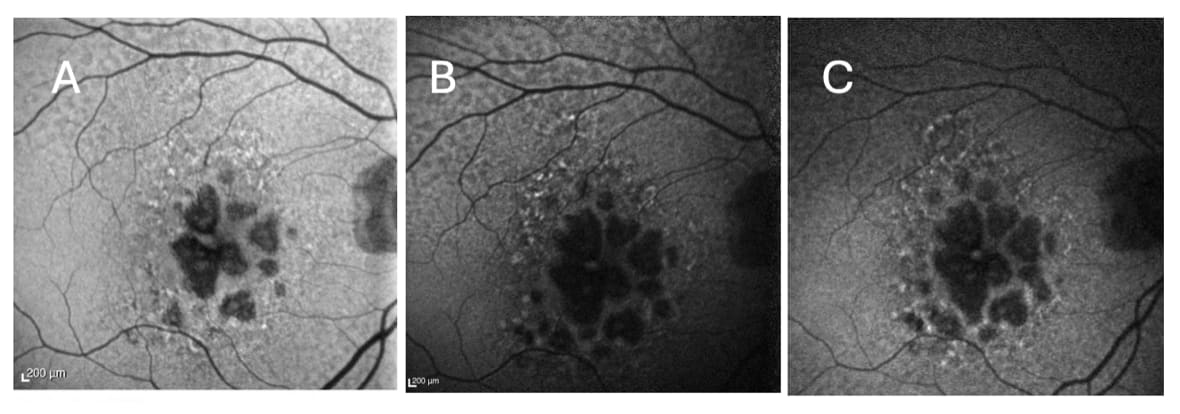
Accurate identification of GA patients is the first step to effective management. While clinical examination often can diagnose GA, optical coherence tomography (OCT) and fundus autofluorescence (FAF) are imperative for monitoring and documenting disease progression.5,6,7 Providing referral sources and educating patients and family members about GA are paramount to ensure they understand its implications on quality of life, progression, and available treatments.
When counseling patients about treatment, it is essential to consider their overall health and potential to benefit from these therapies. The advantages of slowing disease progression should be weighed against the burden of indefinite monthly or bimonthly injections, especially for older patients or those with significant comorbidities. Patients with symptomatic GA, documented GA progression on FAF, experience with intravitreal injections, or significant vision loss are typically more motivated to start and continue treatment (Figure 1).
Treatment Decisions and Follow-Up
Discussing treatment options with complement inhibitors is critical once GA is confirmed. These treatments require frequent office visits for intravitreal injections and necessitate an organized approach to scheduling, patient flow, and follow-up care.4,7 Address potential safety concerns such as intraocular inflammation (IOI), vasculitis, ischemic optic neuropathy (ION), choroidal neovascularization (CNVM), and endophthalmitis with these steps:
- Conduct a thorough consent process.
- Consider treating the worse eye first to monitor for IOI (i.e., first injection phenomenon).
- Avoid treatment in patients with known autoimmune disease.
- Remember treatment is contraindicated in patients with active ocular infection or inflammation.
Resource Management and Team Collaboration
Optimizing resource allocation — including staffing for additional injection appointments, managing drug inventory, and ensuring equipment availability (OCT and FAF) — is crucial as GA management becomes more prevalent. Team collaboration with all staff members working in concert to handle and streamline patient education, follow-up scheduling, and data management for research purposes is key.
Patient Support and Long-term Care
Supporting GA patients extends beyond medical treatment. Integrating low vision services and facilitating education and emotional support through counseling or support groups can address the psychological impact of this chronic condition.9,10 It is important to set realistic expectations about the treatment process, including the need for regular injections, potential side effects, and the importance of long-term adherence.
The introduction of GA treatments has transformed retinal care and requires practices to adapt their office dynamics. By fostering an environment where patients are well-informed and supported throughout their treatment journey, retinal physicians can enhance quality of life significantly for those living with GA.
References:
- Jaffe GJ, Westby K, Csaky KG, et al. C5 inhibitor avacincaptad pegol for geographic atrophy due to age-related macular degeneration: a randomized pivotal phase 3 trial. Ophthalmology. 2021 Apr;128(4):576-586. doi:10.1016/j.ophtha.2020.08.027
- Khanani AM, Patel SS, Staurenghi G, et al. Efficacy and safety of avacincaptad pegol in patients with geographic atrophy (GATHER2): 12-month results from a randomised, double-masked, phase 3 trial. Lancet. 2023 Oct 21;402(10411):1449-1458. doi: 10.1016/S0140-6736(23)01583-0
- Heier JS, Lad EM, Holz FG, et al. Pegcetacoplan for the treatment of geographic atrophy secondary to age-related macular degeneration (OAKS and DERBY): two multicentre, randomised, double-masked, sham-controlled, phase 3 trials. Lancet. 2023 Oct;402(10411):1434-1448. doi:10.1016/S0140-6736(23)01520-9
- Liao DS, Grossi FV, El Mehdi D, et al. Complement C3 inhibitor pegcetacoplan for geographic atrophy secondary to age-related macular degeneration: a randomized phase 2 trial. Ophthalmology. 2020 Feb;127(2):186-195. doi:10.1016/j.ophtha.2019.07.011
- Fleckenstein M, Mitchell P, Freund KB, et al. The progression of geographic atrophy secondary to age-related macular degeneration. Ophthalmology. 2018 Mar;125(3):369-390. doi:10.1016/j.ophtha.2017.08.038
- Sadda SR, Guymer R, Holz FG, et al. Consensus definition for atrophy associated with age-related macular degeneration on OCT: Classification of Atrophy Report 3. Ophthalmology. 2018 Apr;125(4):537-548. doi:10.1016/j.ophtha.2017.09.028
- Holz FG, Sadda SR, Staurenghi G, et al. Imaging protocols in clinical studies in advanced age-related macular degeneration: recommendations from Classification of Atrophy Consensus Meetings. Ophthalmology. 2017 Apr;124(4):464-478. doi:10.1016/j.ophtha.2016.12.002
- Boyer DS, Schmidt-Erfurth U, van Lookeren Campagne M, Henry EC, Brittain C. The pathophysiology of geographic atrophy secondary to age-related macular degeneration and the complement pathway as a therapeutic target. Retina. 2017 May;37(5):819-835. doi:10.1097/IAE.0000000000001392
- Rosenfeld PJ, Dugel PU, Holz FG, et al. Emixustat hydrochloride for geographic atrophy secondary to age-related macular degeneration: a randomized clinical trial. Ophthalmology. 2018 Oct;125(10):1556-1567. doi:10.1016/j.ophtha.2018.03.059
- Sunness JS, Rubin GS, Applegate CA, Bressler NM, Marsh MJ, Hawkins BS, Haselwood D. Visual function abnormalities and prognosis in eyes with age-related geographic atrophy of the macula and good visual acuity. Ophthalmology. 1997 Oct;104(10):1677-1691. doi:10.1016/s0161-6420(97)30079-7

This editorial content was supported via unrestricted sponsorship.