







Antiangiogenesis and antipermeability of pathologic retinal/choroidal vascularization via intravitreal anti–vascular endothelial growth factor (VEGF; formerly known as vascular permeability factor1) agents has had the most dramatic effect in treating the most potentially blinding diseases in Western cultures (Figure 1). The introduction of intravitreal anti-VEGF agents has saved vision in millions of individuals. Challenges remain, however. The relatively brief half-life of anti-VEGF agents dictates that intravitreal administration must be performed frequently, which is often not adhered to in real-world practice.2,3 In addition, treatment refractoriness and resistance to anti-VEGF therapy is still noted in some patients.
The newer anti-VEGF agents have lower molecular weights, which increases the molar equivalent anti-VEGF delivered with each dose. This has proven to increase drying efficacy and durability/duration of action. However, there is a limit to which this property can be effective; also, inflammation tends to occur more often with these agents. Therefore, other pathways besides VEGF that play a role in vascular pathogenesis have been sought to address the vascular pathogenesis.
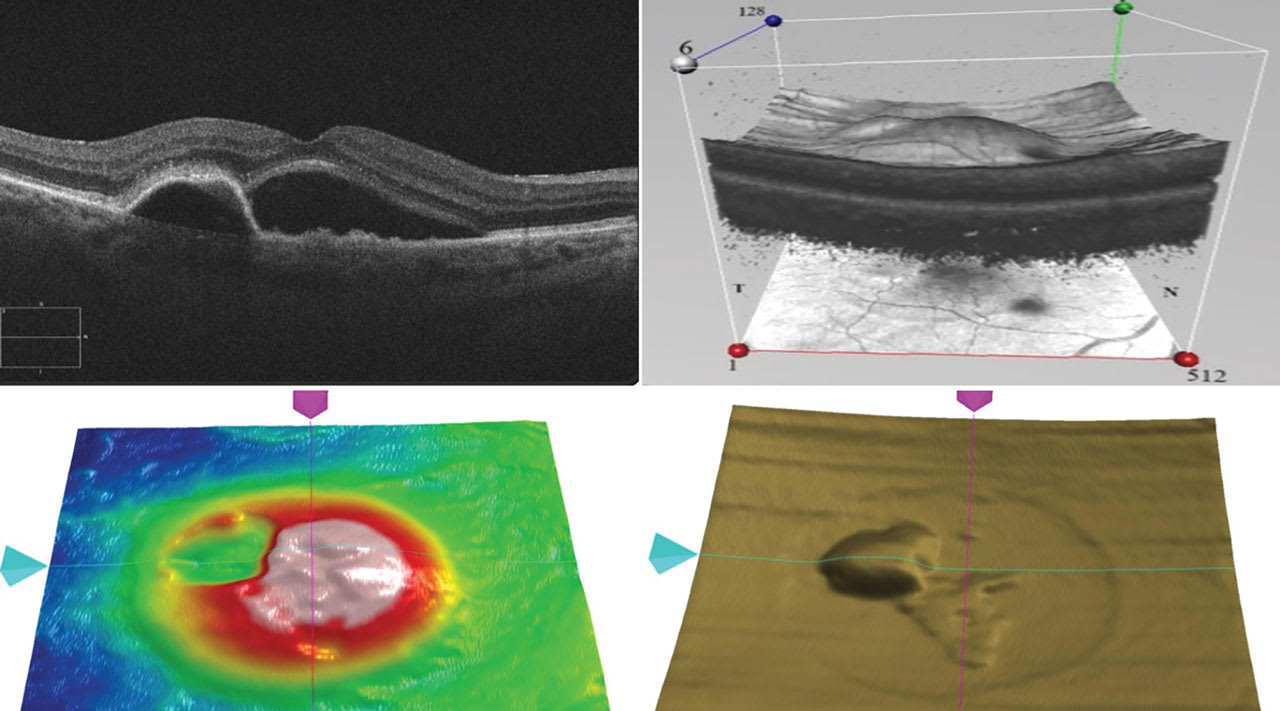
Figure 1. Multiple optical coherence tomography (OCT) images from a single case of neovascular age-related macular degeneration. Clockwise from upper left: subfoveal choroidal neovascularization associated with subretinal fluid and serous pigment epithelial detachment (PED) with a solid component at its anterior border; an image from the “cube” capture of the case, allowing for 3-dimensional analysis of the pathologic anatomy overlying the en face image; the OCT “RPE slab” image showing the PED in relief; the “ILM-RPE” analysis highlights the regions where the fluid is most significant. Image courtesy Michael Colucciello, MD, FASRS.
The angiopoietin-1 (Ang-1)/tyrosine kinase with immunoglobulin and epidermal growth factor homology domains (TIE) pathway has been shown to play an important role in vascular stability. Ang-1 activates the TIE-2 receptor, which promotes vascular stability. Ang-2, up-regulated under pathologic conditions such as ischemia and inflammation, antagonizes Ang-1. Ang-2 in turn inhibits TIE-2 activation, resulting in weakening of endothelial cell junction integrity, vascular instability, recruitment of inflammatory cells, and potentiation of VEGF action, ultimately resulting in increased pathologic vascular permeability. Vitreous levels of Ang-2 are elevated in neovascular age-related macular degeneration (nAMD), diabetic retinopathy (DR), diabetic macular edema (DME), and retinal vein occlusion (RVO).4 Therefore, in theory, adding Ang-2 inhibition to an anti-VEGF agent should improve treatment efficacy compared to anti-VEGF monotherapy.
In the phase 2 RUBY study (NCT02712008), the addition of a separate intravitreal injection of Ang-2 inhibitor nesvacumab (REGN910-3; Regeneron) to intravitreal aflibercept 2 mg (Eylea; Regeneron) demonstrated no additional visual benefit over intravitreal aflibercept monotherapy in DME, although there appeared to be anatomic improvements (better drying and improvement on the Diabetic Retinopathy Severity Scale [DRSS]) at 36 weeks when the combination treatment with higher-dose nesvacumab was given.5,6
Faricimab (Vabysmo; Genentech) is a bispecific antibody that simultaneously neutralizes both Ang-2 and VEGF-A. Faricimab was approved by the FDA for intravitreal use in 2022 based on 2-year phase 3 trial results for YOSEMITE/RHINE (for DME) and TENAYA/LUCERNE (for nAMD). These studies showed that vision gains with faricimab 6.0 mg given up to every 16 weeks remained similar to those achieved with aflibercept 2 mg given every 8 weeks (after loading doses); improved anatomic outcomes observed in YOSEMITE/RHINE with faricimab compared with aflibercept were maintained through 24 months. At year 2, approximately 80% of patients were on faricimab q12w dosing and 60% were on faricimab q16w dosing.7,8
It is encouraging to see evidence of extended durability in the faricimab studies — but was this extended durability, as well as the short-term anatomic improvements seen in RUBY, due to the anti–Ang-2 effect? Or could the perceived durability advantages reported with faricimab be due to the larger dose of anti-VEGF in faricimab (about 2 times greater than aflibercept 2 mg and 4 times greater than ranibizumab 0.5 mg)? Clouding the issue, retinal vascular leakage animal model studies have shown that aflibercept, ranibizumab (Lucentis; Genentech), and brolucizumab (Beovu; Novartis) significantly suppress Ang-2 levels on their own;9 there is controversy as to the translatability of animal models to human disease, however.10
Regarding clinical effect, there was an easier-to-treat population in TENAYA/LUCERNE (higher baseline vision, thinner retinas, and smaller choroidal neovascularization lesions) than typically observed in other trials, which may have accounted for some of the perceived durability advantage in wet AMD.
There are no anti–Ang-2 monotherapies approved for the treatment of retinal diseases. The official prescribing information insert for faricimab states, “the contribution of Ang-2 inhibition to the treatment effect and clinical response for nAMD and DME has yet to be established.”11
Is there convincing evidence that Ang-2 suppression confers any clinical benefit? We are fortunate to have the perspectives of Drs. Arshad M. Khanani and Jennifer I. Lim regarding this important question.
Clinical Trials and Real-world Evidence Show Benefit of Dual Ang-2/VEGF-A Inhibition
Arshad M. Khanani MD, MA, FASRS
Anti-VEGF therapies have had a significant impact on the treatment of retinal diseases such as nAMD, DR, DME, and RVO. Raised VEGF levels in the retina leads to aberrant angiogenesis, vascular permeability, and ultimately retinal disease progression.12-18 However, recent studies have shown that VEGF signaling is only a part of the complex pathophysiology underlying these conditions and preclinical findings indicate the inflammatory cytokine cascade contributes to the disease paradigm.19
Despite the benefits of anti-VEGF treatments, many patients exhibit residual disease activity. For example, in the HAWK and HARRIER trials, 24% to 39% of nAMD patients treated with brolucizumab or aflibercept had retinal fluid after 2 years.20 Similarly, data of patients with DME treated with aflibercept, bevacizumab (Avastin; Genentech), or ranibizumab showed that 44% to 68% had persistent DME at 2 years.21 These findings suggest that alternative pathways contribute to the disease process, necessitating the exploration of additional therapeutic targets.
The Ang-1/TIE-2 pathway is essential for endothelial cell stability and vascular integrity, making it a promising target in retinal pathogenesis. Elevated Ang-2 levels interfere with Ang-1/TIE-2 signaling, promoting vascular instability and inflammation in conditions such as nAMD, DR, PDR, and RVO.4,14,18,22-29 Preclinical models indicate that Ang-2 upregulation results in blood-retinal barrier breakdown, while Ang-2 inhibition stabilizes retinal vessels and reduces inflammation.27
Given the synergistic effects of Ang-2 and VEGF on vascular instability, dual inhibition therapy may offer superior disease control. The RUBY and ONYX trials evaluated the combination of nesvacumab, an Ang-2 inhibitor, with aflibercept, an anti-VEGF agent, in patients with DME and nAMD. Both the RUBY and ONYX studies provided compelling evidence that the combination of nesvacumab and aflibercept significantly improved anatomic outcomes, such as reducing central subfield thickness (CST) and resolving retinal fluid, compared to anti-VEGF monotherapy. These findings support the potential benefits of dual Ang-2 and VEGF inhibition in treating retinal diseases.6,30
Faricimab has shown promising outcomes in clinical trials. The phase 3 YOSEMITE/RHINE clinical trials evaluating faricimab in DME, and TENAYA/LUCERNE evaluating faricimab in nAMD, demonstrated greater reductions in CST and retinal fluid compared to aflibercept.8,31-33 Moreover, in eyes with DME treated with faricimab, a greater reduction of hyperreflective foci (HRF), macular leakage, and epiretinal membrane (ERM) formation was observed when compared to eyes treated with aflibercept.34,35 Faricimab also reduced the presence and thickness of serous pigment epithelial detachments (PEDs) to a greater extent than aflibercept in eyes with nAMD.36,37
Findings from the TRUCKEE study further corroborate the phase 3 clinical trial data. This real-world observational study assessed the efficacy and safety of faricimab in a routine clinical setting. Initial results indicate that faricimab achieved significant improvements in CST and visual acuity, including patients who had suboptimal responses to prior anti-VEGF monotherapy. The study also observed extended dosing intervals, which can reduce treatment burden and improve patient compliance and quality of life.38
The data from both clinical trials and real-world studies, like TRUCKEE, suggest that dual Ang-2/VEGF-A inhibition with faricimab provides superior disease control compared to traditional anti-VEGF monotherapy. Dual inhibition with Ang-2/VEGF-A therapy showed an increased efficacy when treating neovascularization, vascular leakage, inflammation, and proliferative fibrotic disease progression. The dual targeting mechanism of faricimab allowed for faster drying, extended treatment durability, treatment burden reduction, and potentially enhanced patient outcomes and quality of life.
Further research is needed to validate these findings across larger populations and longer follow-up periods. Results from ongoing and future studies exploring the long-term benefits of early initiation with dual pathway inhibitors are needed to further understand the implications on patient outcomes, including visual acuity, treatment adherence, and impact on overall quality of life.
Inhibiting both Ang-2 and VEGF-A pathways appears to offer enhanced control of retinal diseases compared to anti-VEGF monotherapy alone. As we continue to gather evidence through robust clinical trials and real-world studies, the potential benefits of dual pathway inhibition will become clearer, guiding clinicians toward more effective treatment strategies.
Faster Retinal Drying Shown in Imaging Reflects the Beneficial Effect of Ang-2 Inhibition
Jennifer I. Lim, MD, FARVO, FASRS
Ang-2, by binding to the TIE-2 receptor, results in increased endothelial permeability and pericyte detachment from the basement membrane, which contributes to vascular leakage as well as to inflammation, with increased migration of inflammatory cells. Neutralization of Ang-2 stabilizes the TIE-2 receptor by allowing Ang-1 to bind, which leads to vascular stabilization, and decreased permeability of blood vessels.39 Theoretically, inhibition of Ang-2, such as by the bispecific anti-VEGF and anti–Ang-2 antibody faricimab, should contribute to vascular stabilization, with decreased vascular permeability and decreased inflammation. Recent studies provide evidence that the Ang-2 inhibition of faricimab plays an important role in efficacy and durability of faricimab. Clinically, for patients with DME, that translates into reduced exudation and, theoretically, to better drying of the retina.
First, the optical coherence tomography (OCT) imaging data in both phase 3 nAMD and DME clinical trials show better retinal drying with faricimab than with aflibercept, which inhibits VEGF and placental growth factor (PLGF). Prior studies have shown that for an increased anti-VEGF dose alone, as in the HARBOR study for AMD,40 or an aflibercept dose increased by 4 times, as in the PHOTON and PULSAR studies for AMD41 and DME,42 respectively, there is not better drying of the retina as evaluated by OCT imaging. In contrast, the TENAYA and LUCERNE studies of faricimab for AMD,7 and the YOSEMITE and RHINE studies for DME,8 have shown a difference in retinal drying compared to aflibercept 2 mg. During the first 12 weeks of these studies, where patients have received the same number of monthly faricimab or aflibercept 2 mg, the OCT data show better drying for faricimab-treated eyes than aflibercept-treated eyes. Furthermore, the time to achieve first absence of intraretinal fluid and subretinal fluid occurs faster for the faricimab-treated eyes than for the aflibercept-treated eyes.43,44
With harder to treat eyes, such as those with PED, the faricimab-treated eyes in TENAYA and LUCERNE showed greater reductions in PED height than the eyes treated with aflibercept 2 mg.39,45 This supports better drying, which I believe reflects the effect of Ang-2 inhibition.
The clinical benefit of Ang-2 can be seen in real-world data from the FARETINA-AMD database, the Wills Eye database, and the Cleveland Clinic. An overview of these data was presented recently at the Euretina Congress in Barcelona, Spain.46 This faster drying effect also helps explain why faricimab has better durability than other agents. If there is less leakage, there is less fluid present, so retreatment is less often.
Second, in patients with DME, fluorescein angiography (FA) imaging shows a dramatic reduction in the amount of leakage for the eyes treated with faricimab. This decreased permeability helps explain the durability. Hard exudates can be considered a surrogate biomarker for fluid and leakage in DME eyes. An analysis of the YOSEMITE and RHINE studies found faricimab-treated eyes showed a greater reduction in hard exudates, along with OCT central retinal thickness, than eyes treated with aflibercept. In addition, the rate of hard exudate reduction occurred more quickly.47 More recently, volumetric analysis has been evaluated and will be presented at the Macula Society’s 48th meeting February 12-15 in Charlotte Harbor, Florida; these data show greater resolution with the faricimab-treated eyes.
More evidence of the beneficial effect of neutralizing Ang-2 can be found when considering inflammation. OCT analyses of intraretinal hyperreflective foci in DME eyes or subretinal hyperreflective material in AMD eyes show greater reductions in the faricimab-treated eyes compared to the aflibercept-treated eyes.48 In addition, DME eyes treated with faricimab have a lower rate of epiretinal membrane (ERM) formation than in eyes treated with aflibercept.38 This is another example supporting the decreased inflammation seen in faricimab-treated eyes with DME.
In summary, these data show decreased permeability, with better and faster retinal drying, greater resolution of hard exudates, and reduction of inflammatory biomarkers and ERM formation in eyes treated with faricimab compared to eyes treated with aflibercept. The main difference between these 2 treatments is the anti–Ang-2 component. Based on known functions of Ang-2, it is likely that these differences result from the anti–Ang-2 component of faricimab. The data strongly suggest this effect is due to inhibition of Ang-2. RP



References
1. Keck PJ, Hauser SD, Krivi G, et al. Vascular permeability factor, an endothelial cell mitogen related to PDGF. Science. 1989;246(4935):1309-1312. doi:10.1126/science.2479987
2. Ciulla TA, Hussain RM, Pollack JS, Williams DF. Visual acuity outcomes and anti-vascular endothelial growth factor therapy intensity in neovascular age-related macular degeneration patients: a real-world analysis of 49 485 eyes. Ophthalmol Retina. 2020;4(1):19-30. doi:10.1016/j.oret.2019.05.017
3. Ciulla TA, Pollack JS, Williams DF. Visual acuity outcomes and anti-VEGF therapy intensity in diabetic macular oedema: a real-world analysis of 28 658 patient eyes. Br J Ophthalmol. 2021;105(2):216-221. doi:10.1136/bjophthalmol-2020-315933
4. Regula JT, Lundh von Leithner P, Foxton R, et al. Targeting key angiogenic pathways with a bispecific CrossMAb optimized for neovascular eye diseases. EMBO Mol Med. 2016;8(11):1265-1288. doi:10.15252/emmm.201505889
5. Anti-vasculaR endothelial growth factor plUs Anti-angiopoietin 2 in fixed comBination therapY: evaluation for the treatment of diabetic macular edema (RUBY). ClinicalTrials.gov Identifier: NCT02712008. Updated October 3, 2018. Accessed December 4, 2024.
6. Brown DM, Boyer DS, Csaky K, et al. Intravitreal nesvacumab (antiangiopoietin 2) plus aflibercept in diabetic macular edema: phase 2 RUBY randomized trial. Retina. 2022; 42(6):1111-1120. doi:10.1097/IAE.0000000000003441
7. Heier JS, Khanani AM, Quezada Ruiz C, et al. Efficacy, durability, and safety of intravitreal faricimab up to every 16 weeks for neovascular age-related macular degeneration (TENAYA and LUCERNE): two randomised, double-masked, phase 3, non-inferiority trials. Lancet. 2022;399(10326):729-740. doi:10.1016/S0140-6736(22)00010-1
8. Wykoff CC, Abreu F, Adamis AP, et al. Efficacy, durability, and safety of intravitreal faricimab with extended dosing up to every 16 weeks in patients with diabetic macular oedema (YOSEMITE and RHINE): two randomised, double-masked, phase 3 trials. Lancet. 2022;399(10326):741-755. doi:10.1016/S0140-6736(22)00018-6
9. Lange C, Tetzner R, Strunz T, Rittenhouse KD. Aflibercept suppression of angiopoietin-2 in a rabbit retinal vascular hyperpermeability model. Transl Vis Sci Technol. 2023;12(5):17. doi:10.1167/tvst.12.5.17
10. Avery RL, Csaky KG, Westenskow P, Stoilov I, Diack C. Aflibercept does not suppress angiopoietin-2 in patients with nAMD or DME. Transl Vis Sci Technol. 2023;12(10):6. doi:10.1167/tvst.12.10.6
11. Novartis/Roche. Faricimab (VABYSMO) prescribing information. January 2022. Accessed December 4, 2024. https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/761235s000lbl.pdf
12. Nguyen QD, Heier JS, Do DV, et al. The Tie2 signaling pathway in retinal vascular diseases: a novel therapeutic target in the eye. Int J Retina Vitreous. 2020;6:48. doi:10.1186/s40942-020-00250-z
13. Cabral T, Mello LGM, Lima LH, et al. Retinal and choroidal angiogenesis: a review of new targets. Int J Retina Vitreous. 2017;3:31. doi:10.1186/s40942-017-0084-9
14. Joussen AM, Ricci F, Paris LP, Korn C, Quezada-Ruiz C, Zarbin M. Angiopoietin/Tie2 signalling and its role in retinal and choroidal vascular diseases: a review of preclinical data. Eye (Lond). 2021;35(5):1305-1316. doi:10.1038/s41433-020-01377-x
15. Witmer AN, Vrensen GF, Van Noorden CJ, Schlingemann RO. Vascular endothelial growth factors and angiogenesis in eye disease. Prog Retin Eye Res. 2003;22(1):1-29. doi:10.1016/s1350-9462(02)00043-5
16. Uemura A, Fruttiger M, D’Amore PA, et al. VEGFR1 signaling in retinal angiogenesis and microinflammation. Prog Retin Eye Res. 2021;84:100954. doi:10.1016/j.preteyeres.2021.100954
17. Khanani AM, Russell MW, Aziz AA, et al. Angiopoietins as potential targets in management of retinal disease. Clin Ophthalmol. 2021;15:3747-3755. doi:10.2147/OPTH.S231801
18. Khan H, Aziz AA, Khanani Z, et al. Approved treatments for neovascular age-related macular degeneration: current safety and future directions. Expert Opin Drug Saf. 2024;23(9):1109-1114. doi:10.1080/14740338.2024.2387318
19. Canonica J, Foxton R, Garrido MG, et al. Delineating effects of angiopoietin-2 inhibition on vascular permeability and inflammation in models of retinal neovascularization and ischemia/reperfusion. Front Cell Neurosci. 2023;17:1192464. doi:10.3389/fncel.2023.1192464
20. Hussain RM, Neal A, Yannuzzi NA, et al. Brolucizumab for persistent macular fluid in neovascular age-related macular degeneration after prior anti-VEGF treatments. Ther Adv Ophthalmol. 2021;13:25158414211055964. doi:10.1177/25158414211055964
21. Bressler NM, Beaulieu WT, Glassman AR, et al. Persistent macular thickening following intravitreal aflibercept, bevacizumab, or ranibizumab for central-involved diabetic macular edema with vision impairment: a secondary analysis of a randomized clinical trial. JAMA Ophthalmol. 2018;136(3):257-269. doi:10.1001/jamaophthalmol.2017.6565
22. Saharinen P, Eklund L, Alitalo K. Therapeutic targeting of the angiopoietin-TIE pathway. Nat Rev Drug Discov. 2017;16(9):635-661. doi:10.1038/nrd.2016.278
23. Mandriota SJ, Pepper MS. Regulation of angiopoietin-2 mRNA levels in bovine microvascular endothelial cells by cytokines and hypoxia. Circ Res. 1998;83(8):852-859. doi:10.1161/01.res.83.8.852
24. Rangasamy S, Srinivasan R, Maestas J, McGuire PG, Das A. A potential role for angiopoietin 2 in the regulation of the blood-retinal barrier in diabetic retinopathy. Invest Ophthalmol Vis Sci. 2011;52(6):3784-3791. Published 2011 Jun 1. doi:10.1167/iovs.10-6386
25. Collazos-Alemán JD, Gnecco-González S, Jaramillo-Zarama B, Jiménez-Mora MA, Mendivil CO. The role of angiopoietins in neovascular diabetes–related retinal diseases. Diabetes Ther. 2022;13(11-12):1811-1821. doi:10.1007/s13300-022-01326-9
26. Hammes HP, Lin J, Wagner P, et al. Angiopoietin-2 causes pericyte dropout in the normal retina: evidence for involvement in diabetic retinopathy. Diabetes. 2004;53(4):1104-1110. doi:10.2337/diabetes.53.4.1104
27. Park DY, Lee J, Kim J, et al. Plastic roles of pericytes in the blood-retinal barrier. Nat Commun. 2017;8:15296. doi:10.1038/ncomms15296
28. Wong HL, Fung NSK, Kwok AKH. Brolucizumab and faricimab as new treatment options for diabetic macular edema: perspective. Hong Kong J Ophthalmol. 2022;26:53-57.
29. Larsen HO, Grauslund J, Vergmann AS. Efficacy, Durability and Safety of Faricimab in Neovascular Age-Related Macular Degeneration and Diabetic Macular Oedema: Lessons Learned from Registration Trials. Ophthalmol Ther. 2023;12(5):2253-2264. doi:10.1007/s40123-023-00753-6
30. Heier JS, Ho AC, Boyer DS, et al. Intravitreal nesvacumab (anti-angiopoietin-2) plus aflibercept in neovascular AMD: phase 2 ONYX randomized trial. J Vitreoretin Dis. 2022;7(1):8-15. doi:10.1177/24741264221126061
31. Khan M, Aziz AA, Shafi NA, Abbas T, Khanani AM. Targeting angiopoietin in retinal vascular diseases: a literature review and summary of clinical trials involving faricimab. Cells. 2020;9(8):1869. doi:10.3390/cells9081869
32. Penha FM, Masud M, Khanani ZA, et al. Review of real-world evidence of dual inhibition of VEGF-A and ANG-2 with faricimab in NAMD and DME. Int J Retina Vitreous. 2024;10(1):5. doi:10.1186/s40942-024-00525-9
33. Chaudhary V, Kotecha A, Willis JR, et al. Individualized faricimab dosing up to every 16 weeks maintains robust anatomic and vision outcomes through 2 years in nAMD. Presented at: Association for Research in Vision and Ophthalmology annual meeting; New Orleans, LA; April 23-27, 2023.
34. Maunz A, von Schulthess E, Patel K, et al. Automated segmentation of hyperreflective foci in diabetic macular edema shows greater volume reduction by faricimab vs aflibercept in phase 3 YOSEMITE and RHINE. Presented at: Association for Research in Vision and Ophthalmology annual meeting; New Orleans, LA; April 23-27, 2023.
35. Jaffe GJ, Ogura Y, Deák G, et al. Impact of faricimab vs aflibercept on epiretinal membrane formation over 2 years in eyes with DME in the YOSEMITE/RHINE phase 3 trials. Presented at: American Society of Retina Specialists annual meeting; Seattle, WA; July 27-August 1, 2023.
36. Lim JI, Margaron P, Souverain A, et al. Greater reduction in pigment epithelial detachment size with faricimab vs aflibercept during head-to-head dosing in patients with nAMD. Presented at: the 56th Retina Society annual scientific meeting; New York, NY; October 11-14, 2023.
37. Lai TYY, Khanani AM, Souverain A, Yang M, Patel S, Margaron P. Greater reduction in pigment epithelial detachment size with faricimab vs aflibercept during head-to-head dosing in patients with neovascular age-related macular degeneration. Presented at: 16th Asia-Pacific Vitreo-Retina Society Congress; Hong Kong; December 8-10, 2023.
38. Khanani AM, Aziz AA, Khan H, et al. The real-world efficacy and safety of faricimab in neovascular age-related macular degeneration: the TRUCKEE study — 6-month results. Eye (Lond). 2023;37(17):3574-3581. doi:10.1038/s41433-023-02553-5
39. Chakravarthy U, Bailey C, Brown D, et al. Phase 1 trial of anti–vascular endothelial growth factor/anti-angiopoietin 2 bispecific antibody RG7716 for neovascular age-related macular degeneration. Ophthalmol Retina. 2017;1(6):474-485. doi:10.1016/j.oret.2017.03.003
40. Ho AC, Busbee BG, Regillo CD, et al. Twenty-four-month efficacy and safety of 0.5 mg or 2.0 mg ranibizumab in patients with subfoveal neovascular age-related macular degeneration. Ophthalmology. 2014;121(11):2181-2192. doi:10.1016/j.ophtha.2014.05.009
41. Brown DM, Boyer DS, Do DV, et al. Intravitreal aflibercept 8 mg in diabetic macular oedema (PHOTON): 48-week results from a randomised, double-masked, non-inferiority, phase 2/3 trial. Lancet. 2024;403(10432):1153-1163. doi:10.1016/S0140-6736(23)02577-1
42. Lanzetta P, Korobelnik JF, Heier JS, et al. Intravitreal aflibercept 8 mg in neovascular age-related macular degeneration (PULSAR): 48-week results from a randomised, double-masked, non-inferiority, phase 3 trial. Lancet. 2024;403(10432):1141-1152. doi:10.1016/S0140-6736(24)00063-1
43. Lim JI. Anti-VEGF/anti–Ang-2 year 2 outcomes for diabetic macular edema and neovascular AMD. Presented at: the American Academy of Ophthalmology 2022 Retina Subspeciality Day; Chicago, IL; September 30-October 3, 2022.
44. Lim JI. Targeting Ang-2 and VEGF: biology, pharmacokinetics, and latest clinical data in nAMD and DME. Presented at: Angiogenesis, Exudation, and Degeneration 2024 Virtual Congress; February 3, 2024.
45. Lim JI, Margaron P, Souverain A, et al. How effective is anti–Ang-2 and anti-VEGF (faricimab) for neovascular AMD with pigment epithelial detachments? Presented at: the American Academy of Ophthalmology 2023 Retina Subspeciality Day; San Francisco, CA; November 3-6, 2023.
46. Lim JI, Tabano D, Ferhina A, et al. 12-month real-world clinical and anatomical outcomes with faricimab in patients with neovascular age-related macular degeneration: FARETINA-AMD. Presented at: the 24th EURETINA Congress; Barcelona, Spain; September 19-22, 2024.
47. Lim JI. Faricimab vs aflibercept in the reduction of exudates in Y/R trials. Presented at: Clinical Trials at the Summit; Park City, Utah; June 8, 2024.
48. Downey L, Sivaprasad S, Chhabra R, et al. Dual pathway inhibition with faricimab for previously treated neovascular age-related macular degeneration and diabetic macular oedema: guidance from a UK panel of retina specialists. Eye (Lond). 2024;38(16):3077-3086. doi:10.1038/s41433-024-03223-w