







Notal Vision’s Scanly home OCT device allows patients with neovascular age-related macular degeneration (nAMD) to perform daily self-operated scans. These are analyzed by a proprietary, AI-based software that interprets the images and provides key insights into retinal fluid accumulation. Physicians can review patient data through a HIPAA-compliant web portal.
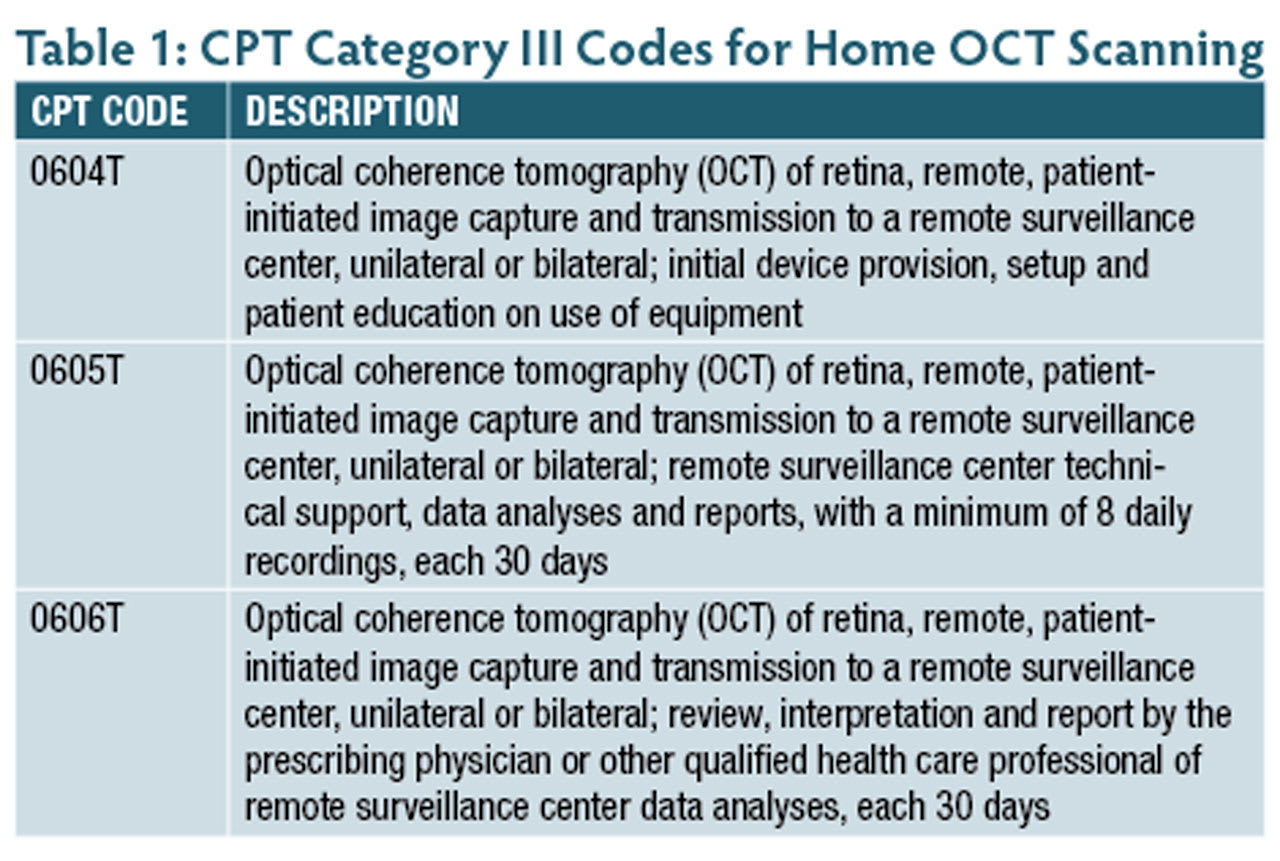
The AMA’s Current Procedural Terminology (CPT) Editorial Panel has created 3 Category III CPT codes related to home OCT scanning: 0604T, 0605T, and 0606T (Table 1). The Notal Vision remote monitoring center bills for the initial setup and patient education (0604T) and the capture and transmission of the data from the remote retina OCT (0605T) with at least 8 daily recordings every 30 days. Physicians can bill 0606T once every 30 days if they have performed and documented the interpretation and report (I&R) of the captured data.
Q. What is a Category III CPT code?
A. Category III codes are for new services, procedures, and technologies. Using a Category III code to collect data on these new services and procedures is essential to identify the emerging services, procedures, technology, and service models for outcomes and utilization. If there is an appropriate Category III code, it must be used instead of an unlisted Category I code. The Medicare Administrative Contractor prices Category III codes because there isn’t an established fee schedule. Category III codes are billed to the patient’s insurance or the patient.
Q. Can I count time spent reviewing patient images as part of the E/M service when I next see that patient?
A. No, the time needed to review the images taken by home OCT is built into the 0606T code.
Q. Can the practice bill 99457 and 99458 with, or instead of, 0606T?
A. No. The Notal Vision center that sets up and trains the patient to use the equipment performs the remote monitoring. Both 99457 and 99458 indicate that the practice would conduct the monitoring. The practice would only bill 0606T when the physician performs an I&R that should be documented in the patient’s medical record, just as for an I&R for a diagnostic test performed in the office.
Q. What are the documentation requirements for billing 0606T?
A. Test results interpretation should include a detailed analysis of the remote OCT scan findings, including measurements of retinal layer thicknesses, presence of abnormalities, and any significant changes from previous readings, and how the information will be used in the patient’s treatment plan.
Q. Because Category III codes don’t have an established fee schedule, what comparable code(s) would be used to determine a fee?
A. Because the physician only provides an I&R, consider using the retina OCT as a comparable code for the baseline fee. The comparison should only include the professional component, not the technical component, because the physician or the practice did not provide the scan. RP
