







Anti–vascular endothelial growth factor (anti-VEGF) therapy has revolutionized the management of neovascular age-related macular degeneration (nAMD). Just 2 decades ago, a diagnosis of nAMD typically meant patients would lose an average of 3 lines of vision within a year, with limited treatment options available.1 Today, however, most newly diagnosed nAMD patients can experience significant vision improvement after just a few doses of anti-VEGF therapy. With continued treatment, many can maintain these gains indefinitely, barring other outcomes such as subfoveal geographic atrophy.
The modern anti-VEGF era (Figure 1) began with the approval of ranibizumab 0.5 mg (Lucentis; Genentech) for nAMD in 2006. Around the same time, bevacizumab (Avastin; Genentech), initially approved for cancer treatment, was used off-label for nAMD due to its similar mechanism of action and significantly lower cost. Another early anti-VEGF treatment, pegaptanib sodium injection (Macugen; OSI Eyetech Pharmaceuticals/Pfizer), was approved in 2004. Although Macugen targeted VEGF165 specifically, it was eventually overshadowed by the more potent anti-VEGF therapies that followed. (Macugen is no longer available in the United States.)
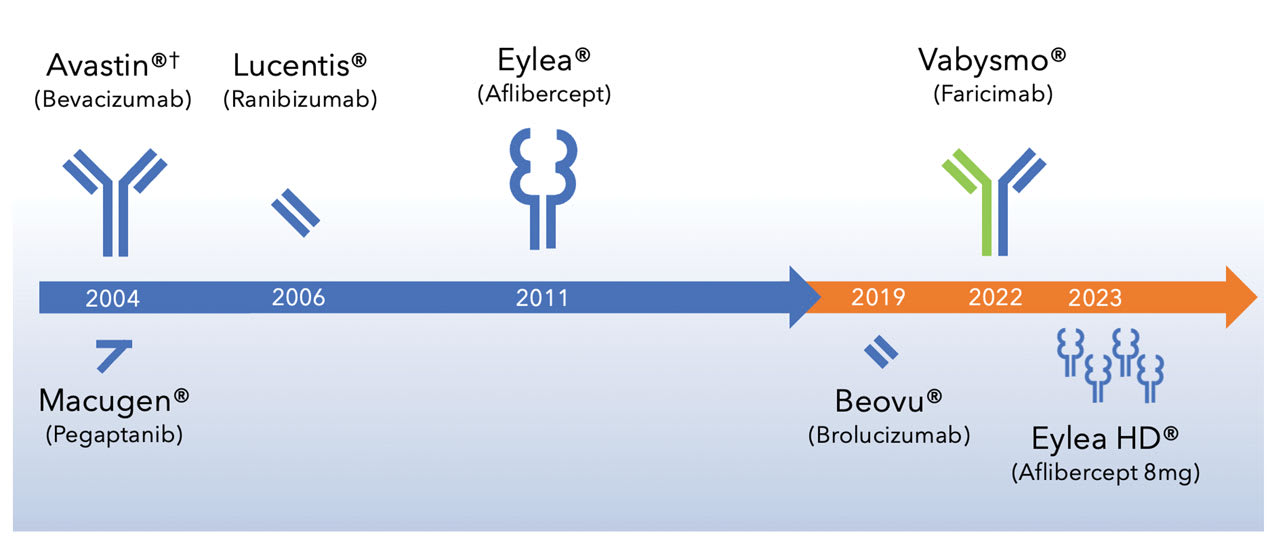
Figure 1. Development timeline for first-generation and second-generation anti-VEGF therapies for neovascular age-related macular degeneration. Image courtesy Scott D. Walter, MD, MSc.
†Avastin was approved in 2004 for metastatic colon cancer, and subsequently for other cancer indications. It has never been FDA approved for nAMD or for intraocular use.
In 2011, aflibercept 2 mg (Eylea; Regeneron) was approved, offering similar efficacy with the added benefit of extended dosing intervals (every 8 weeks after 3 initial monthly doses). Aflibercept quickly gained popularity among retina specialists, and by 2018, it controlled approximately 50% of the global anti-VEGF market for nAMD.
Although first-generation anti-VEGF therapies provided substantial visual benefits, the frequent injections required posed a considerable treatment burden. To address this, second-generation anti-VEGF agents were developed to extend durability, improve fluid reduction, and reduce the need for injections while maintaining visual outcomes and safety. Brolucizumab 6 mg (Beovu; Novartis), faricimab-svoa 6 mg (Vabysmo; Genentech), and aflibercept 8 mg (Eylea HD; Regeneron) are FDA-approved second-generation anti-VEGF agents that have reshaped the treatment landscape for nAMD.
Comparative Pharmacology
A distinguishing feature of second-generation anti-VEGF agents is their higher “molar dose” compared to Eylea (Figure 2). Brolucizumab is a humanized single-chain variable fragment monoclonal antibody targeting VEGF-A. Its smaller molecular size and higher molar concentration (6.0 mg/0.05 mL) allow for deeper retinal penetration and greater binding capacity compared to first-generation agents. With a molecular weight of 26 kDa, brolucizumab has 12.7 times the molar concentration of Eylea.
Vabysmo is a bispecific antibody, the first of its kind for intraocular use. Its structure is most like Avastin but also targets angiopoietin-2 (Ang-2) in addition to VEGF-A. Although Vabysmo has a higher molar dose than Eylea (2.2 times), only half of its binding capacity is dedicated to VEGF-A. Thus, its effective VEGF-A binding is nearly equivalent to that of Eylea. The primary difference between Vabysmo and Eylea lies in Vabysmo’s dual targeting of VEGF-A and Ang-2, which may enhance fluid control and improve clinical outcomes.
Eylea HD is a high-dose formulation of aflibercept (8.0 mg/0.07 mL), offering 4 times the molar dose of conventional Eylea (2.0 mg/0.05 mL). Despite the higher concentration, Eylea HD’s mechanism remains the same as the original formulation. Aflibercept acts as a decoy receptor for VEGF-A, VEGF-B, and placental growth factor (PlGF). Aflibercept has a much higher binding affinity for VEGF-A than other anti-VEGF agents, which may explain its superior effectiveness in reducing retinal fluid. The lower dissociation constant (KD) of aflibercept means it binds VEGF-A more tightly, removing the VEGF load from the eye more quickly.
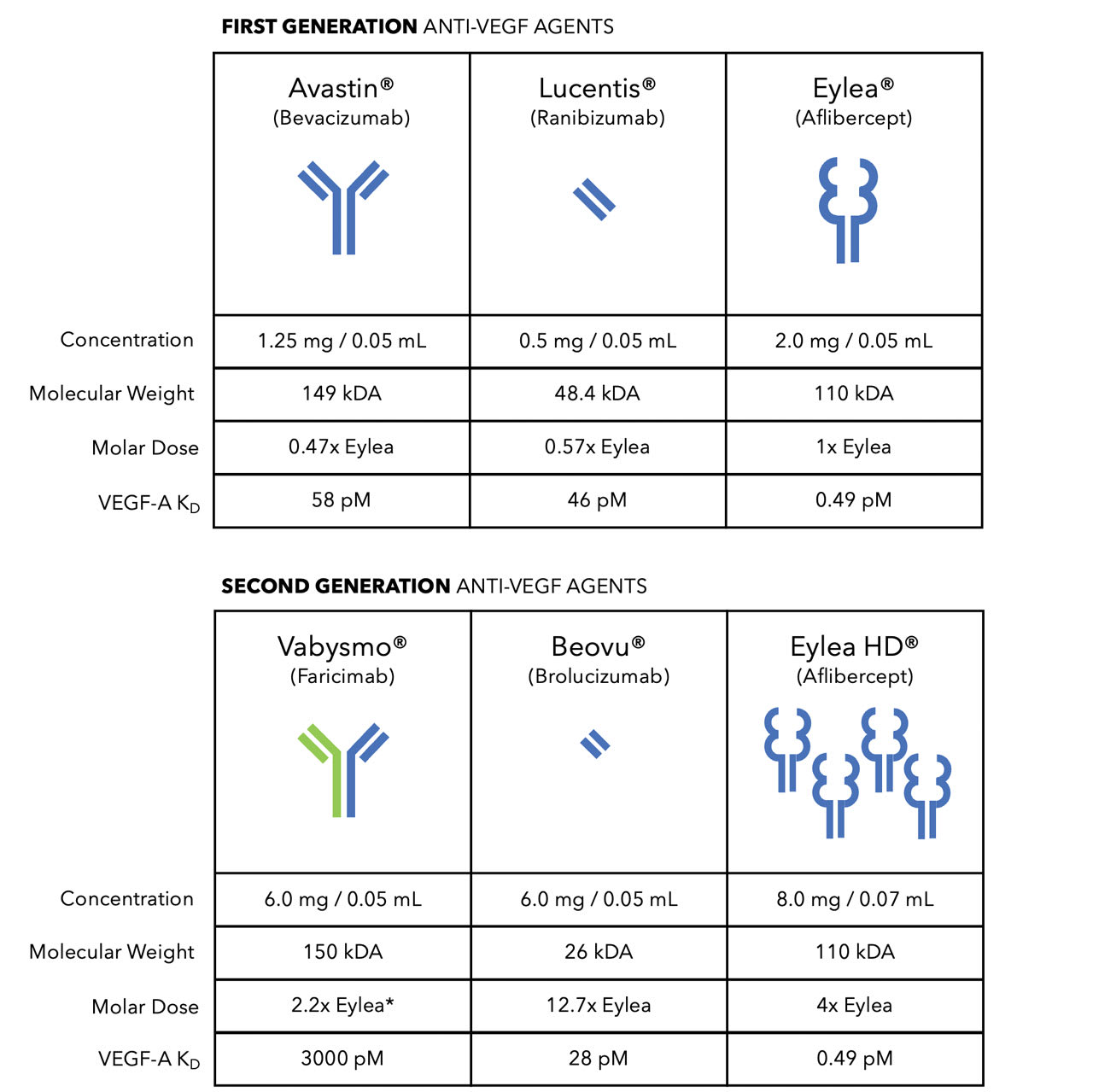
Figure 2. Comparative pharmacology of first-generation and second-generation anti-VEGF agents. Image courtesy Scott D. Walter, MD, MSc.
* Vabysmo is a bispecific antibody with binding sites for VEGF-A and Ang-2. Although the molar dose of Vabysmo is 2.2 times the molar dose of Eylea, the effective molar dose is 1.1 times, because only half of its binding capacity is dedicated to VEGF-A.
Vabysmo has a relatively lower binding affinity for VEGF-A (KD=3,000 pM) compared to Eylea (KD=0.49 pM), but this may confer an advantage. Vabysmo’s lower affinity allows for continuous binding and release of VEGF-A, providing a buffering effect over time. In contrast, aflibercept’s stronger, almost irreversible binding to VEGF-A results in rapid reduction of VEGF load immediately after an injection, but decreased VEGF binding availability over time.
One of the unique features of aflibercept, the active ingredient in Eylea and Eylea HD, is its “fully human” molecular structure. Unlike other anti-VEGF agents, which are “humanized”—meaning they are derived from both human and mouse protein sequences—aflibercept is considered fully human because all its amino acid sequences occur naturally in the human body. It is a recombinant fusion protein that combines the extracellular domains of human VEGF receptors 1 and 2 with the Fc portion of human IgG. The fully human nature of aflibercept may contribute to its relatively low immunogenicity, meaning it is less likely to provoke an immune response compared to other anti-VEGF therapies.
Clinical Trial Data
The efficacy of Beovu, Vabysmo, and Eylea HD has been demonstrated in multiple clinical trials. In the HAWK and HARRIER trials, Beovu showed noninferiority to Eylea in terms of visual acuity (VA) gains and superior reduction in central subfield thickness (CST) at 48 weeks, with the added benefit of the potential for longer injection intervals (every 12 weeks after 3 loading doses).2 Beovu was particularly effective in patients with more severe disease or greater fluid burden at baseline, with superior fluid control compared to Eylea.
In the TENAYA and LUCERNE trials, Vabysmo demonstrated noninferiority to Eylea in VA gains at 48 weeks.3 Additionally, Vabysmo offered extended dosing intervals (every 8 to 16 weeks) based on patient response after 4 initial monthly doses. Post hoc analyses indicated that Vabysmo’s dual VEGF-A and Ang-2 targeting enhanced fluid control, with faster elimination of retinal fluid in Vabysmo-treated eyes, with fewer injections than Eylea.4
In PULSAR, Eylea HD demonstrated noninferiority to standard Eylea in maintaining VA and reducing CST, with the added benefit of longer dosing intervals (12 or 16 weeks after 3 loading doses).5 Secondary analyses revealed that Eylea HD achieved better fluid reduction compared to conventional Eylea, particularly in patients with more severe disease.
Real-World Experience
Saba and Walter (2023) analyzed real-world outcomes from 1,438 brolucizumab injections in 626 nAMD eyes, revealing significant reductions in macular volume and CST, with the elimination of intraretinal fluid (IRF), subretinal fluid (SRF), and serous pigment epithelium detachments (PEDs) in most patients.6 However, they also observed a relatively high rate of intraocular inflammation, including retinal vasculitis, and retinal vascular occlusion. These safety concerns have been echoed by others, limiting the widespread adoption of brolucizumab despite its promising fluid control.7,8
The TRUCKEE study examined faricimab’s real-world efficacy, showing average VA gains of 5-6 letters at 6 months.9 Among patients switched from aflibercept 2 mg, 18.5% showed elimination of IRF and 26.6% eliminated SRF after a single faricimab injection. After 6 faricimab injections, these numbers increased to 24.1% and 31.1%, respectively, underscoring faricimab’s potential for enhanced fluid control.
The FARETINA study, which included over 9,500 eyes, confirmed that Vabysmo significantly reduced CST and improved fluid control in both treatment-naïve and previously treated nAMD patients.10 Patients switched to Vabysmo after more than 12 months of prior anti-VEGF therapy saw a decrease in CST from 295 µm to 276 µm after the first Vabysmo injection, with continued reductions over time.
Although no real-world studies on Eylea HD have been published, early reports suggest it provides promising results. Tallo and Walter (2025) analyzed 61 eyes switched to Eylea HD due to suboptimal responses with standard Eylea.11 After 3 injections of Eylea HD, the median dosing interval increased from 6.0 weeks to 9.7 weeks. Visual and anatomical outcomes remained stable, suggesting that Eylea HD is effective for patients who struggle with conventional treatments.
One concern with Eylea HD is its higher injection volume (0.07 mL vs the standard 0.05 mL). Edwards and Walter (2024) found no significant difference in immediate post-injection intraocular pressure (IOP) between standard and HD doses, though IOP took slightly longer to return to baseline after Eylea HD injections.12
Summary
Large randomized trials for Beovu, Vabysmo, and Eylea HD have demonstrated that these second-generation anti-VEGF therapies are noninferior to Eylea, with extended dosing intervals and potential for improved fluid control. Real-world studies further support these findings, with second-generation agents offering enhanced anatomic efficacy and durability, especially in patients with severe disease. However, real-world safety concerns, particularly with Beovu, have limited its use. The safety, efficacy, and durability of Vabysmo has been well established in large real-world studies like TRUCKEE and FARETINA. Early real-world data on Eylea HD are promising, although its higher injection volume may raise IOP concerns for certain patients. The introduction of second-generation anti-VEGF agents has significantly altered the treatment landscape for nAMD, reducing the treatment burden for many patients while continuing to achieve excellent visual outcomes. RP


References
1. Arnold J, Blumenkranz M, Bressler NM, et al. Photodynamic therapy of subfoveal choroidal neovascularization in age-related macular degeneration with verteporfin: one-year results of 2 randomized clinical trials—TAP report. Arch Ophthalmol. 1999;117(10):1329-1345. doi:10.1001/archopht.117.10.1329
2. Dugel PU, Koh A, Ogura Y, et al. HAWK and HARRIER: phase 3, multicenter, randomized, double-masked trials of brolucizumab for neovascular age-related macular degeneration. Ophthalmology. 2020;127(1):72-84. doi:10.1016/j.ophtha.2019.04.017
3. Heier JS, Khanani AM, Quezada Ruiz C, et al. Efficacy, durability, and safety of intravitreal faricimab up to every 16 weeks for neovascular age-related macular degeneration (TENAYA and LUCERNE): two randomised, double-masked, phase 3, non-inferiority trials. Lancet. 2022;399(10326):729-740. doi:10.1016/S0140-6736(22)00010-1
4. Pitcher J, Gallego-Pinazo R, Amador M, et al. Association of early fluid resolution with short- and long-term extended durability in the head-to-head phase of the TENAYA/LUCERNE trials in patients with neovascular age-related macular degeneration treated with faricimab. Presented at: the 57th Retina Society annual meeting; September 11-15, 2024; Lisbon, Portugal.
5. Lanzetta P, Korobelnik JF, Heier JS, et al. Intravitreal aflibercept 8 mg in neovascular age-related macular degeneration (PULSAR): 48-week results from a randomised, double-masked, non-inferiority, phase 3 trial. Lancet. 2024;403(10432):1141-1152. doi:10.1016/S0140-6736(24)00063-1
6. Saba NJ, Walter SD. Efficacy, safety, and durability of brolucizumab: an 8-month post-marketing surveillance analysis. Clin Ophthalmol. 2023;17:2791-2802. doi:10.2147/OPTH.S425709
7. Baumal CR, Spaide RF, Vajzovic L, et al. Retinal vasculitis and intraocular inflammation after intravitreal injection of brolucizumab. Ophthalmology. 2020;127(10):1345-1359. doi:10.1016/j.ophtha.2020.04.017
8. Witkin AJ, Hahn P, Murray TG, et al. Occlusive retinal vasculitis following intravitreal brolucizumab. J Vitreoretin Dis. 2020;4(4):269-279. doi:10.1177/2474126420930863
9. Khanani AM, Aziz AA, Khan H, et al. The real-world efficacy and safety of faricimab in neovascular age-related macular degeneration: the TRUCKEE study—6 month results. Eye (Lond). 2023;37(17):3574-3581. doi:10.1038/s41433-023-02553-5
10. Ali FS, Bonine NG, Leng T, et al. Real-world clinical outcomes update in patients with neovascular age-related macular degeneration in the US: the FARETINA-AMD study. Presented at: Hawaiian Eye and Retina 2025 meeting; January 18-24, 2025; Kauai, Hawaii.
11. Tallo C, Walter SD. Switching from aflibercept 2mg to 8mg in eyes with “difficult-to-treat” neovascular AMD. Abstract submitted to ASRS 2025 annual meeting.
12. Edwards CM, Walter SD. Serial tonometry following intraocular injections: how does injection volume affect IOP? Paper presented at: American Academy of Ophthalmology annual meeting; October 17-21, 2024; Chicago.