







Age-related macular degeneration (AMD) represents a significant public health challenge, with an estimated 288 million cases projected globally by 2040.1 Vision loss from AMD affects critical activities such as reading, mobility, and driving, while also contributing to emotional and psychological challenges, including depression.2
Socioeconomic disparities in health care access and utilization have compounded the burden of vision-threatening AMD (VT-AMD), consisting of exudative AMD and atrophic nonexudative AMD. Individuals of lower socioeconomic status (SES) or from socioeconomically deprived areas are more likely to present with advanced disease stages.3 However, limited research has explored disparities in eye care utilization among AMD patients. This study aims to investigate how socioeconomic status (SES) influences eye care utilization for VT-AMD patients, identify the barriers these patients face, and propose strategies to improve access to care.
Study Overview
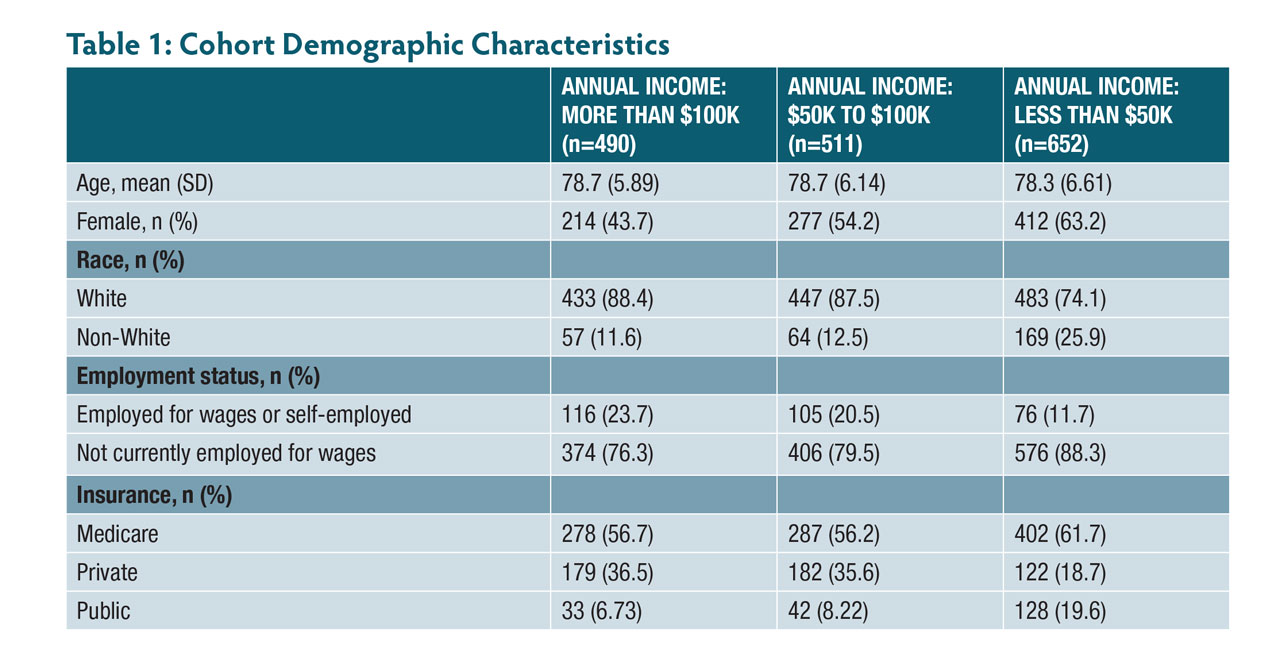
Data for the study were sourced from the National Institutes of Health’s All of Us Research Program, which includes diverse populations, with a particular focus on those underrepresented in biomedical research. The dataset spans 2010 to 2023 and includes self-reported demographics, diagnostic codes for VT-AMD, and data on eyecare utilization (Table 1).
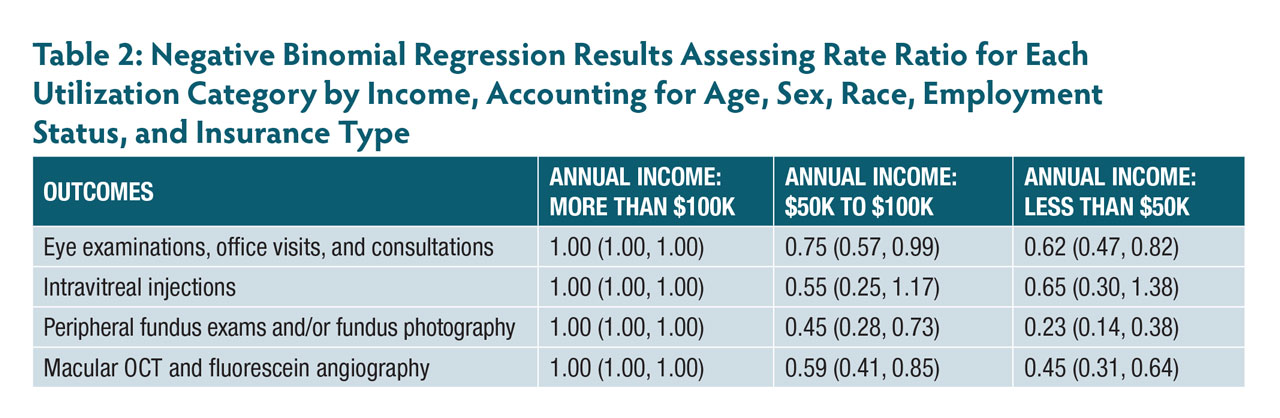
The cohort consisted of individuals aged 65 years or older who had been diagnosed with VT-AMD, as identified by ICD-9 or ICD-10 codes. Outcomes of interest included utilization metrics such as eye examinations, intravitreal injections, and diagnostic imaging procedures like optical coherence tomography (OCT). The frequency of utilization metrics was calculated per 100 person-years. Negative binomial regression models were used to assess the relationship between income levels and eyecare utilization, with adjustments for demographic and clinical variables.
Key Findings
Participants earning $50,000 to $100,000 annually exhibited 25% lower rates of eye examinations, 55% lower rates of peripheral fundus exams and fundus photography, and 41% lower rates of macular OCT and fluorescein angiography compared to those earning more than $100,000 annually. The disparities were even more pronounced for participants with an annual income below $50,000, who had 38% lower rates of eye examinations, 77% lower rates of fundus photography, and 55% lower rates of macular OCT and fluorescein angiography. Despite these significant disparities, there were no observed differences in intravitreal injection rates across income brackets (Figure 1, Table 2).
Barriers to Eye Care
Several factors contribute to the underutilization of eye care services among low-income VT-AMD patients. Anti–vascular endothelial growth factor (anti-VEGF) therapies, essential for treating neovascular AMD, are costly. This financial strain often results in delayed or incomplete treatment, compromising patient outcomes.4 Low-income individuals often face longer wait times, fewer follow-up appointments, and limited access to ophthalmologists, particularly in underserved areas. Public health care settings may also offer fewer resources compared to private practices. Health care system barriers also play a significant role in restricting access. In underserved areas, there are fewer ophthalmologists, and public health care settings generally have longer wait times and less frequent follow-up appointments compared to private practices.5 These challenges are compounded by mobility issues because many low-income individuals live in areas with limited access to specialized care and lack reliable transportation.4,6

Figure 1. Utilization rates in 100 person-years by annual income. Image courtesy Ji Yun Han, BS.
Recommendations and Conclusion
To address these barriers and improve access to care for VT-AMD patients, several strategies can be implemented. Patient assistance programs (PAPs) sponsored by pharmaceutical companies can provide access to essential medications, including anti-VEGF therapies, at little or no cost to eligible patients. Studies have shown that PAPs can improve medication adherence and health outcomes.7 Additionally, the adoption of telemedicine can facilitate remote monitoring and follow-up care. This approach is particularly beneficial for patients facing transportation challenges.8
The study highlights significant income-related disparities in eye care utilization among VT-AMD patients. By implementing targeted interventions, including financial assistance programs and telemedicine solutions, we can ensure equitable access to eye care and enhance the quality of life for all VT-AMD patients, regardless of their socioeconomic status.

References
1. Wong WL, Su X, Li X, et al. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: a systematic review and meta-analysis. Lancet Glob Health. 2014;2(2):e106-16. doi:10.1016/S2214-109X(13)70145-1
2. Fleckenstein M, Keenan TDL, Guymer RH, et al. Age-related macular degeneration. Nat Rev Dis Primers. 2021;7(1):31. doi:10.1038/s41572-021-00265-2
3. Levinger N, Beykin G, Grunin M, et al. Socioeconomic status and visual outcome in patients with neovascular age-related macular degeneration. Eur J Ophthalmol. 2021;31(3):1094-1100. doi:10.1177/1120672120920783
4. More P, Almuhtaseb H, Smith D, Fraser S, Lotery AJ. Socio-economic status and outcomes for patients with age-related macular degeneration. Eye (Lond). 2019;33(8):1224-1231. doi:10.1038/s41433-019-0393-3
5. Nguyen V, Daien V, Guymer RH, et al. Clinical and social characteristics associated with reduced visual acuity at presentation in Australian patients with neovascular age-related macular degeneration: a prospective study from a long-term observational data set. The Fight Retinal Blindness! Project. Clin Exp Ophthalmol. 2018;46(3):266-274. doi:10.1111/ceo.13038
6. Choi A, Nawash BS, Du K, Ong J, Chhablani J. Barriers to care in neovascular age-related macular degeneration: current understanding, developments, and future directions. Surv Ophthalmol. 2024;69(1):160-164. doi:10.1016/j.survophthal.2023.09.001
7. Johnson PE. Patient assistance programs and patient advocacy foundations: alternatives for obtaining prescription medications when insurance fails. Am J Health Syst Pharm. 2006;63(21 Suppl 7):S13-S17. doi:10.2146/ajhp060464
8. Ramchandran RS, Yilmaz S, Greaux E, Dozier A. Patient perceived value of teleophthalmology in an urban, low income US population with diabetes. PLoS One. 2020;15(1):e0225300. doi:10.1371/journal.pone.0225300