







Traditional fundus photography has been enhanced by advances in resolution and widefield and ultrawidefield imaging. Optical coherence tomography (OCT), which characterizes anatomy and pathologic fluid accumulation in histologic detail, has undergone a number of improvements as we have progressed from time-domain to spectral-domain to swept-source Fourier domain acquisition. The longer wavelength of the swept-source OCT (SS-OCT) compared to spectral-domain OCT (SD-OCT) allows for deeper tissue penetration, which yields better visualization of retinal pigment epithelium (RPE) and sub-RPE lesions. The tunable swept laser source in SS-OCT allows for faster scanning, denser (improved) resolution, and larger scan areas than SD-OCT.
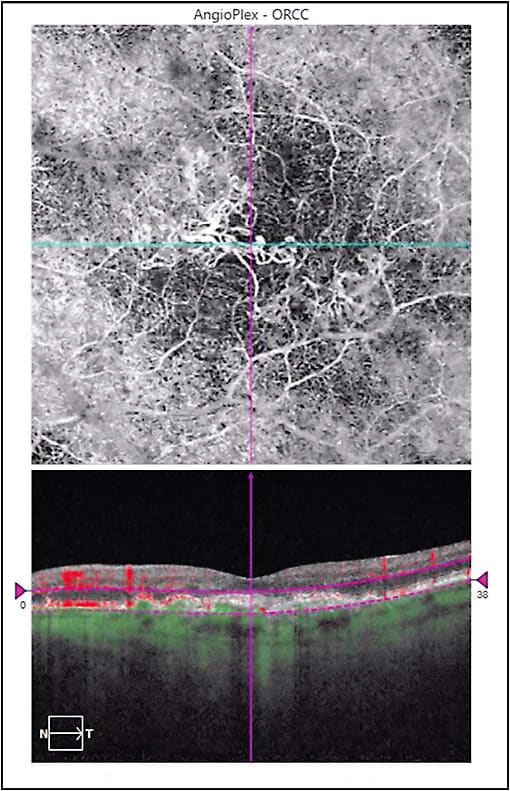
OCT angiography (OCTA) is a noninvasive method that uses red blood cell phase decorrelation technology with high frequency scanning to indirectly visualize blood vessels in a 3-dimensional manner, revealing the trilaminar (superficial, intermediate, and deep) retinal capillary plexus, areas of retinal capillary nonperfusion, intraretinal microvascular abnormalities, and retinal neovascularization. In addition, OCTA can show pathologic choroidal neovascularization (CNV) (Figure 1), and it may discriminate type 1 from types 2 and 3 CNV. Limitations include inability to visualize lesions with slow flow, like retinal microaneurysms and polyps in polypoidal choroidal vasculopathy. Because there is no interference from leakage (which is not detected), vascular anatomy can be shown in stunning detail.
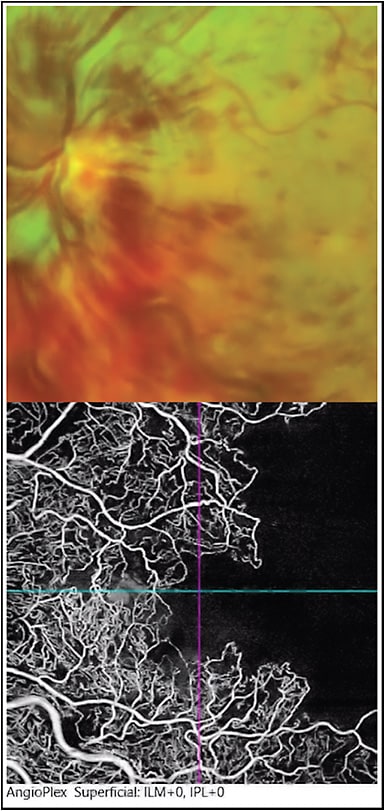
Fluorescein angiography (FA), which was first introduced in the 1960s, continues to be utilized to characterize retinal circulation and permeability in retinal vascular disease and identify active leakage in CNV. Because anti-VEGF pharmacotherapy has been shown to be superior to focal laser photocoagulation of retinal microvascular issues and CNV, FA is not utilized as much as in the past to delineate pathology, but it is useful for baseline diagnosis. Widefield FA is popular for identifying ischemia and neovascularization in the mid-periphery and periphery (Figure 2). Indocyanine angiography (ICG) complements FA in assessing deeper lesions, such as polyps in idiopathic polypoidal choroidal vasculopathy and CNV below subretinal hemorrhage. Fundus autofluorescence (FAF) can reveal the health of the RPE and detect the buildup of lipofuscin, which is highly autofluorescent. FAF is useful in following progression of geographic atrophy in age-related macular degeneration and monitoring of choroidal inflammatory disease.
In the future, we can look forward to further advances, such as characterization of photoreceptor health with adaptive optics. How can we utilize advances that have occurred in imaging to most efficiently manage our patients with exudative maculopathies? This month, we are fortunate to have commentary by Mark H. Nelson, MD, MBA, regarding this important consideration.
Multimodality Imaging in Exudative Maculopathy
Mark H. Nelson, MD, MBA
Exudative maculopathies, most commonly manifested as exudative age-related macular degeneration, diabetic macular edema, and retinal vein occlusion, can be visualized by ophthalmic examination; however, historically, these pathologies have been imaged using an invasive dye technique, intravenous fluorescein angiography. Complementing this study is OCT, which allows for quantifying exudation, most commonly used to monitor treatment effect.
The vast majority of the landmark clinical trials for retinal disease have used these 2 techniques; they have been adopted as “standard of care” imaging techniques. In addition, the vast majority of these diseases are mediated through vascular endothelial growth factor (VEGF), therefore allowing for the “successes” of anti-VEGF agents.
However, what would happen if these standards were not “good enough?” What would happen if researchers found additional biomarkers to determine efficacy of treatments? What would happen if payers demanded more cost-effective treatment? What is the value and utility of newer techniques, specifically ICG videoangiography or OCTA? Is there a nuanced need to do these tests? Or should they be standard parts of treatment paradigms?
I argue that we need to be doing more imaging, not less. We are entering into an era of personalized medicine. The field of oncology is leveraging biomarkers and genetic tests to segment patients for successful targeted therapy. Segmenting patients can provide additional value for ophthalmology by creating new targets and markets for innovative treatments.
My recent Retinal Physician article1 showed that patients with exudative maculopathies with subretinal exudation often have 2 pathological processes — choroidal hyperpermeability and angiogenesis. To treat these patients correctly, ICG imaging is critical. Indocyanine green is also critical to determining the presence of polypoidal disease, for which photodynamic therapy in combination with an anti-VEGF agent may be superior to anti-VEGF monotherapy alone.2 The use of OCTA is becoming mandatory to successfully treat patients with exudative maculopathies, by showing range of neovascularization from subtle vessels within an area of occult membrane to arteriolarized neovascularization, which has been shown to be insensitive to VEGF withdrawal in animals and clinically in humans.
We are in an environment of declining reimbursements for imaging and therapeutic interventions. The question then is do we continue down the path of commoditization where all patients are treated the same or do we find better treatment paradigms that are more cost effective and have higher quality and value? I propose creating segments of disease populations through innovative imaging techniques that will provide more value for the 4 stakeholders in our industry: patients, providers, payers, and pharmaceutical companies. RP
REFERENCES
- Nelson MH. Pachychoroid and exudative maculopathy. Retin Physician. 2020;17(4):18-23.
- Koh A, Lai TYY, Takahashi K, et al. Efficacy and safety of ranibizumab with or without verteporfin photodynamic therapy for polypoidal choroidal vasculopathy: a randomized clinical trial. JAMA Ophthalmol. 2017;135(11):1206-1213.