







Throughout our medical and surgical training, we’re all exposed to absolutes and truisms from our senior mentors and colleagues. Eventually, we discover that some of these absolutes may have been based on outright myths, anecdotal experiences, or come from obsolete data that have since changed due to newer diagnostic or therapeutic modalities.
Here, we present five misconceptions and clinical pearls regarding common vitreoretinal presentations that you’ve probably heard or seen during your training or early years of clinical practice.
1 The presence of a Weiss ring always indicates a complete posterior vitreous detachment (PVD) from the retina.
Usually, but not always, the presence of a Weiss ring indicates a complete PVD. Normally, the vitreous separates in a posterior-to-anterior fashion, possibly causing traction on the peripheral retina, which can lead to a retinal flap or tear. This dynamic process may subsequently allow vitreous fluid into the subretinal space, leading to an acute rhegmatogenous retinal detachment.
We have previously shown that, not uncommonly, you can find a triamcinolone-stained residual layer of vitreous (i.e., the posterior hyaloid) still attached to the posterior and peripheral retina in eyes presenting with a preexisting PVD and an acute retinal detachment.1
In these cases of retinal detachment with an actual “incomplete” PVD, the equatorial and anterior vitreous (or hyaloid) is detached over one large proportion of the retina, but remains attached in the other areas of the retina. This can occur in up to 7% of rhegmatogenous retinal detachments.1 More specifically, the posterior hyaloid is usually separated from the quadrant(s) with retinal breaks, but remains adherent in areas of attached retina (Figure 1).
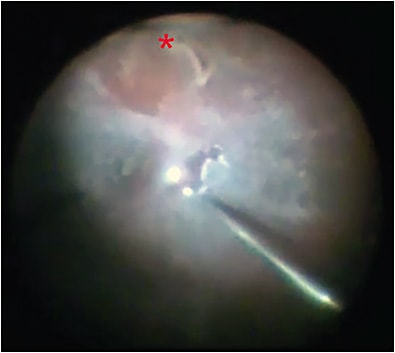
There is significant debate as to whether this residual layer represents an incomplete PVD, vitreoschisis, or immature proliferative vitreoretinopathy (PVR) membrane formation secondary to PVR.2,3 While this debate will surely continue, the use of chromovitrectomy with diluted intravitreal triamcinolone allows for easy, reliable, and consistent identification of the adherent vitreous layer on the retinal surface. Inducing a complete separation of the vitreous and hyaloid to the underlying peripheral retina for 360 degrees is paramount to executing an effective vitrectomy and minimizing the risk of secondary PVR.
2 All retinal detachments are an emergency.
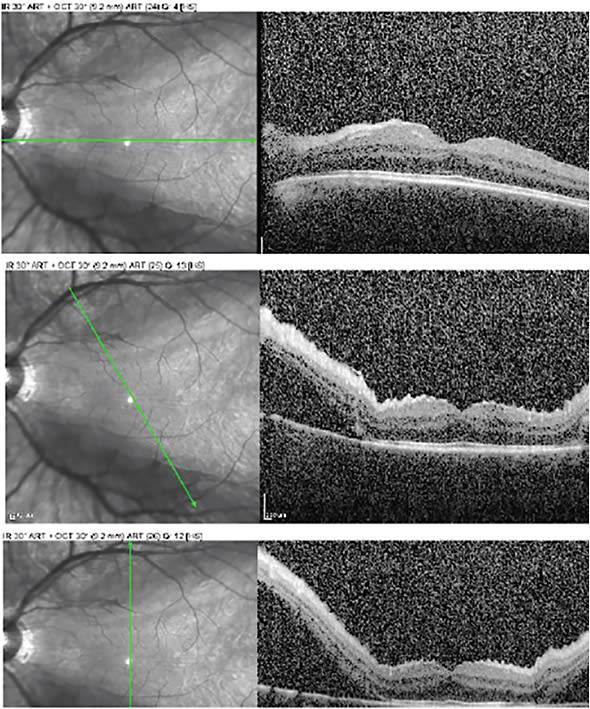
Rhegmatogenous retinal detachments should be considered a surgical urgency; however, this doesn’t apply to all retinal detachments. We’re often asked ‘is the macula on or off?’ but the real key to determining the urgency of a case should be whether or not the fovea is attached. This isn’t always readily apparent clinically, especially when shallow fluid is present. However, OCT imaging enables us to more objectively determine the status of the fovea and/or the extent of macula involvement.
Figure 2 shows what we have termed a “fovea-sparing macula-off” rhegmatogenous retinal detachment. There is evidence that the macula is detached. In addition, the OCT shows subretinal fluid present in the superior and inferior macular area, shallow retinal folds secondary to subretinal fluid, and a high watermark above the fovea, suggesting relative chronicity. However, one can consider this an urgency, because the fovea remains attached and the presenting visual acuity was 20/25 for this patient; consequently, without urgent surgical reattachment, there is significant risk of vision loss.
In addition, the presence of risks factors for rhegmatogenous retinal detachment can help with determining the urgency of a surgical case. Relevant risk factors include age, retinal detachment in the fellow eye, high myopia, family history, lattice degeneration, trauma, cataract surgery (0.6% - 1.7% annual risk), and posterior capsule status.4
For example, a monocular patient who had a sudden onset of flashes and floaters with a fovea-splitting superotemporal retinal detachment may be an emergent case. Conversely, an asymptomatic patient with subretinal fluid leading up to, but not beyond, the inferior retinal vascular arcades (with or without a demarcation line) could potentially be scheduled as an elective case.
Finally, a careful scleral-depressed, dilated fundoscopic examination is key. The clinician should consider cases of asymptomatic chronic retinal detachment where the retinal breaks may have self-barricaded with pigment, pseudophakic high myopes with small retinal breaks that are difficult to examine in the office or that may be hiding within retinal folds in the case of a bullous detachment, non-progressive peripheral degenerative retinoschisis, and exudative retinal detachments secondary to neoplastic or inflammatory disease. All of these require different levels of urgency and management that should be taken into consideration.
3 White dots in the posterior pole are always due to inflammation.
While we all like to hunt zebras and identify white dot syndromes, focal white lesions in the posterior pole are probably more commonly due to inflammatory or neoplastic diseases. Of importance is the early recognition of the manifestations of metastatic disease. Metastatic lesions are the most common intraocular tumor in adults; autopsy studies show up to 12% of cancer patients have choroidal metastatic disease and, in breast cancer, the incidence of choroidal metastasis approaches 40%.5
Choroidal metastasis occurs secondary to hematogenous dissemination with the choroid being the most common ocular site, followed by the iris/ciliary body, retina, and optic nerve. Most choroidal metastatic lesions are carcinomas, and one-third of patients don’t have a known cancer history.
For males, the primary cancer site is usually lung (40%), unknown (30%), gastrointestinal (10%), kidney, prostate, and skin. For females, breast (70%), lung (10%), unknown (10%), gastrointestinal, skin, and kidney are most common. Approximately 11% of patients with choroidal metastatic lesions are asymptomatic; those with symptoms tend to be non-specific: blurred vision (70%), flashes and floaters (12%), and pain (7%). The prognosis is unfortunately poor with a mean life expectancy of 9 to 10 months.
Multimodality treatment is usually required and may consist of systemic chemotherapy, hormone therapy, external beam radiation, brachytherapy, proton beam radiation, and, in some cases, surgery.
Metastatic lesions are relatively flat, ill-defined, and usually creamy yellow in color (Figure 3). They may have overlying retinal pigment epithelium changes (“leopard spotting”) and be associated with exudative retinal detachment when chronic. These lesions are classically bilateral and multifocal, but surprisingly are seen in only 25% of cases.
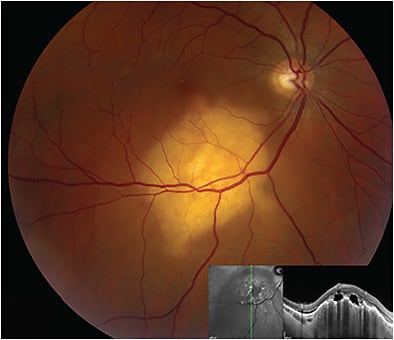
On echography, A-scan shows a moderate-high internal reflectivity and B-scan displays ill-defined choroidal masses with possible lobulated components. Fluorescein angiography is rarely useful to differentiate these from other pathogenic processes, but may show early hypofluorescence with late hyperfluorescence.
4 Topical corticosteroids are fine to use in patients presenting with intraocular inflammation.
When considering intraocular inflammation and a possible uveitic diagnosis, first rule out infectious processes. Topical corticosteroids, especially if used in high doses or for a long duration, can alter the clinical course of an infectious presentation and confound or delay diagnosis.
Be on the lookout for these red flags when a patient presents with intraocular inflammation:
- First episode in an elderly patient
- Significant systemic illness and comorbidities
- Recent hospitalization with indwelling catheters
- Recent bowel surgery
- Existing systemic immunosuppression due to medical therapy
- Existing HIV or AIDS, or engaging in high-risk behavior that increases the risk of contracting HIV or AIDS
- Substance abuse disorders.
These patients won’t present in typical ways and can progress very quickly. Moreover, they require a very high index of suspicion for an infectious process. The indiscriminate use of topical or intravitreal corticosteroids can cost valuable time in the management of these challenging cases.
We advise careful workup, close observation, and detailed counseling for any patient who presents with intraocular inflammation and any of these red flags. It is also helpful to comanage these individuals with a primary care provider, or, in some cases, a rheumatologist and infectious disease specialist.
5 Viral vectors for gene therapy are not safe.
In the early 2000s, after several serious setbacks in the use of viral vectors for gene therapy, there was significant concern about the viability of gene replacement therapy using viral vectors.6 Now, with the recent approval of voretigene neparvovec-rzyl (Luxturna, Spark Therapeutics), an adenovirus-associated virus therapy for bi-allelic RPE65 inherited retinal dystrophy, there is hope that viral vectors will provide an ideal route for the treatment of inherited retinal disease. Perhaps, in the future, such therapy will also be readily available for more common gene-associated degenerative retinal diseases, such as age-related macular degeneration.
Bi-allelic RPE65 retinal dystrophy presents with severe visual impairment before age 1 and is associated with nystagmus, poor pupillary reflexes, normal or mildly abnormal fundus appearance, and profoundly abnormal or absent electroretinogram.7-9 Phenotype varies from a normal fundus appearance to RPE granularity, vessel attenuation, macular coloboma, “salt-and-pepper” retinopathy, and nummular pigmentation.10-12
Although absent of the RPE65 gene, there is preservation of all retinal layers, making it an ideal disease for gene replacement therapy. With viral vectors, the correct DNA is transfected into the RPE via adeno-associated virus. The Luxturna clinical trials show that gene replacement therapy with viral vectors is safe and effective with potential for long-term efficacy. NRP
REFERENCES
- Chin EK, Almeida DRP, Folk JC. Letter to the editor: posterior hyaloid removal. Ophthalmic Surg Lasers Imaging Retina. 2015;46(4):404.
- Kuriakose RK, Xu K, Chin EK, Almeida DRP. Proliferative vitreoretinopathy (PVR) update: current surgical techniques and emerging medical management. J Vitreoretin Dis. 2017;1(4):261-269.
- Xu K, Chin EK, Parke DW, Almeida DRP. Epiretinal membrane and cystoid macular edema as predictive factors of recurrent proliferative vitreoretinopathy. Clin Ophthalmol. 2017;11:1819-1824.
- Lois N, Wong D. Pseudophakic retinal detachment. Surv Ophthalmol. 2003;48(5):467-487.
- Jardel P, Sauerwein W, Olivier T, et al. Management of choroidal metastases. Cancer Treat Rev. 2014;40(10):1119-1128.
- Thomas CE, Ehrhardt A, Kay MA. Progress and problems with the use of viral vectors for gene therapy. Nat Rev Genet. 2003;4(5):346-358.
- Rohen JW, Rentsch FJ. Elektronenmikroskopische Untersuchungen über den Bau der Außenwand des Schlemmschen Kanals unter besonderer Berücksichtigung der Abflußkanäle und Altersveränderungen. Graefes Archiv fur Ophthalmol. 1969;117(15):1-17.
- Franceschetti A, Dieterle P. Diagnostic and prognostic importance of the electroretinogram in tapetoretinal degeneration with reduction of the visual field and hemeralopia. Confin Neurol. 1954;14(2-3):184-186.
- Franceschetti A. Rubéole pendant la grossesse et cataracte congénitale chez l’enfant, accompagnée du phénomène digito-oculaire. Ophthalmologica. 1947;114:332-339.
- Leighton DA, Harris R. Retinal aplasia in association with macular coloboma, keratoconus and cataract. Clin Genet. 1973;4(3):270-274.
- Margolis S, Scher BM, Carr RE. Macular colobomas in Leber’s congenital amaurosis. Am J Ophthalmol. 1977;83(1):27-31.
- Francois J. Choroideremia (progressive chorioretinal degeneration). Int Ophthalmol Clin. 1968;8(4):949-964.

