







In 2001, the Age-Related Eye Disease Study (AREDS) research group announced the beneficial effects of a combination of antioxidant vitamins (vitamins C, E, and beta-carotene) and minerals (zinc and copper) on reducing the risk of progression to late age-related macular degeneration (AMD) by 25% in 5 years.1 Although the clinical trial ended then with a median follow-up of 6.5 years, the participants were followed for an additional 5 years until 2005 to provide natural history of a chronic condition that progresses slowly. Further analyses at 10 years of follow-up in participants with AREDS categories 3 and 4 at baseline demonstrated a significant reduction in the risk of progressing to late AMD (odds ratio [OR] 0.66; 95% confidence interval [CI], 0.53-0.83).2 The development of moderate vision loss (a decrease of 3 or more lines of vision compared with baseline) was also reduced in those participants who were assigned to the AREDS supplements (OR 0.71; 95% CI, 0.57-0.88). No adverse effects associated with the AREDS formulation were seen at 10 years. Mortality was reduced in participants assigned to zinc, especially death from circulatory diseases. Thus, despite stopping the randomized clinical trial, the data at 10 years demonstrated a statistically significant reduction in the risk of developing late AMD and the risk of its accompanying visual loss.
AREDS2
In 2006, the original 11 AREDS clinical sites were joined by 71 other community and academic clinical sites of retinal specialists to form the AREDS2 research group, which evaluated the addition of lutein/zeaxanthin and omega-3 long-chain polyunsaturated fatty acids to the original AREDS. Observational data from AREDS and numerous other studies suggest that these 2 nutritional factors may be important for AMD. The AREDS2 investigators also tested the elimination of beta-carotene and reduction of the zinc level to 25 mg. The study was restricted to participants with bilateral large drusen or late AMD in 1 eye. The results reported in 2013 demonstrated that omega-3 fatty acids (1 g) did not have either a beneficial or harmful effect.3 Substitution of lutein (10 mg) and zeaxanthin (2 mg) for beta-carotene was warranted because beta-carotene was found to increase the risk of lung cancer twofold, especially in those participants who were former smokers. The combination of lutein and zeaxanthin was found to have incremental beneficial effect, especially in those participants who had the lowest dietary intake of lutein and zeaxanthin and when lutein/zeaxanthin were compared head-to-head with beta-carotene, ranging from an additional 20% to 25% increased reduction.
It is now more about 10 years since the AREDS2 study was initiated. Selected AREDS2 clinical sites are re-examining the AREDS2 participants to provide further information on the status of their AMD at 10 years of follow-up. Additional information may help to understand the natural course of AMD in this new era of anti-VEGF therapies and more intensive systemic therapies for cardiovascular disease with antihypertensive drugs and cholesterol-lowering drugs, such as statins.
GENETICS AND AMD
In 2005, one of the first genome-wide association studies was conducted on 196 AREDS participants and complement factor H (CFH), a genetic variant, which was found to be associated with AMD.4 This was confirmed by several groups of investigators. Since then, new data regarding the genetic associations with AMD has increased exponentially. A large international AMD genetic consortium has reported on 52 genetic variants in 34 loci to be associated with AMD in 16,114 AMD cases and 17, 832 controls.5 This new knowledge may be very helpful in determining the pathogenesis of AMD. The different pathways associated with these genetic variants may also define potential targets for treatment. Genetic testing is particularly important for a better understanding of the biology underlying AMD.
Klein et al tested the hypothesis that genetic variants may influence how patients respond to AREDS supplements.6 They found that some differences may exist, but all participants regardless of the genotype responded to the AREDS supplements. They suggested no genetic testing should be done prior to starting the AREDS supplements. Awh et al evaluated the AREDS data and concluded that genetic testing is important because CFH variants were identified to interact negatively with response to zinc, resulting in harmful effects.7 The AREDS research group also conducted analyses of genetic interaction with response to the AREDS supplements, but they failed to find a statistically significant interaction.8 They found that all genotypes responded to the AREDS supplements. Disagreements are not uncommon in science. A recent analysis by 3 independent volunteer groups of statisticians could not replicate the claims of the genotype-treatment interaction.9 They found errors in the challengers’ data. The 3 arbitrating statistical groups also found that the high-risk participants particularly benefited from the AREDS supplements. The 3 teams of statistical experts recommended that patients who meet the criteria for treatment should be offered the AREDS supplements without considering genotyping. These recommendations are similar those of the American Academy of Ophthalmology.10
THE STATUS OF AREDS/AREDS2 SUPPLEMENTATION
After decades of research in antioxidant vitamins and minerals for AMD, how is the AREDS2 supplement used in the community? How has this research been translated to real practice? Recently, Retinal Physician conducted a survey to evaluate the current patterns of use and to understand the barriers associated with recommendations of this treatment. The questions were directed to treating retinal physicians. A description of the questions and the results of the analyses are found in the table. The survey received 66 responses. This may not be entirely representative of the general treating physicians in the United States. Despite these limitations, there are some lessons learned.
KNOWLEDGE REGARDING THE SUPPLEMENTS
The treating physicians were queried about their knowledge of the xanthophyll lutein and its various related components such as zeaxanthin and mesozeaxanthin. It should be noted that he AREDS and AREDS investigators tested only lutein and zeaxanthin, so they have no data to comment on the use of mesozeaxanthin. However, it is known through studies of monkeys that once lutein is consumed, the body converts the lutein to mesozeaxanthin as well. The effects of these various components on the progression to late AMD is unknown, because such a study would require a very large sample size.
TREATMENT INDICATIONS
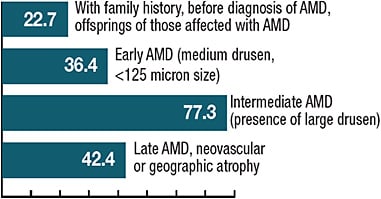
It is reassuring that 90% of the treating physicians feel comfortable in the identification of those patients who clearly have indications for use of the AREDS2 supplements. According to the results of the survey, physicians generally treated according to the AREDS/AREDS2 guidelines which recommend AREDS2 supplements for those with intermediate AMD (bilateral large drusen) or those with late AMD in 1 eye. A surprising proportion of the treating physicians also recommended the supplements at the earlier stages, such as early AMD or those with family history (and possibly no evidence of AMD). It may be important for those with early AMD or with positive family history to have regular eye exams for evaluation of the onset of AMD or more severe stages. This could result in better counseling of careful self-monitoring as well as emphasizing the use of the supplements.
BARRIERS TO TAKING AREDS2 SUPPLEMENTS
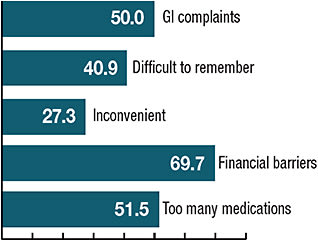
It is not surprising that the patients’ comorbidities may create some challenges, because the number of medications required for these patients may be quite high in this elderly population. Failing memory also poses a problem for patients taking the AREDS2 supplements. Furthermore, the financial burden can also restrict their ability to obtain the supplements. The gastrointestinal intolerance to the supplement can also reduce the number of patients who can take the supplements regularly. Some patients find that they can take the individual components and often delete the zinc to avoid these adverse side effects.
IMPLEMENTATION OF TRANSLATIONAL RESEARCH
Retinal Physician has conducted an interesting survey to help us understand some of the barriers. We still need to understand how well such translational research has been implemented. We recognize from other areas of medicine that it often requires long periods of time to translate information from clinical trials. Perhaps with the current research in the IRIS registry managed by the American Academy of Ophthalmology, we may be able to obtain a more “real world” assessment of the indications, use, and perhaps barriers to the use of AREDS2 supplements for the treatment of AMD. We look forward to such analyses.
Supplement Survey Responses
Retinal Physician conducted a short survey of its readership regarding use of and challenges of eye health supplementation.
Below are the questions and responses.

- Do you consider every lutein supplement to be equal (i.e. mesozeaxanthin, zeaxanthin lutein, etc.)?
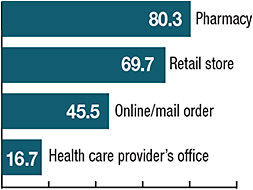
- Where do your patients get their supplements/vitamins? (Check all that apply.)
- At what point in the disease progression do you suggest the patient take the supplement? (Check all that apply.)
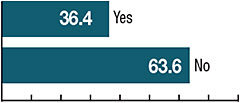
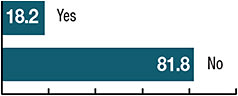
- Do you find patient selection a challenge?
- What reasons do patients give for noncompliance? (check all that apply.)
- Do you believe it is ethical for health care providers to sell supplements in their offices?
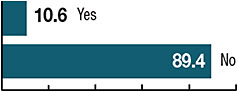
- Do you sell supplements in your office?
SUMMARY
After decades of research in nutritional supplements in AREDS and AREDS2, we still need to understand how to overcome barriers to providing suppplements to patients who have indications for treatment. The report from the National Academies of Science, Engineering, and Medicine issued in September 2016 proposed a number of steps that could facilitate the translation of research findings to benefit the Americans affected with eye diseases through public health initiatives and engaging the state and local communities to promote and encourage eye- and vision-heathy environments.11 Hopefully, some of the recommendations will be implemented in the future to help with translation of all research findings from researchers in the vision and ophthalmology. RP
REFERENCES
- Age-Related Eye Disease Study Group. A randomized, placebo-controlled clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report no. 8. Arch Ophthalmol. 2001;119(10):1417-1436.
- Chew EY, Clemons TE, Agron E, et al; the Age-Related Eye Disease Study Group. Long-term effects of vitamins C, E, and beta-carotene, and zinc on age-related macular degeneration. AREDS report no. 35. Ophthalmology. 2013;120(8):1604-1611.
- Age-Related Eye Disease Study 2 Research Group. Lutein + zeaxanthin and omega-3 fatty acids for age-related macular degeneration: the Age-Related Eye Disease Study 2 Research group. JAMA. 2013;309(19):2005-2015.
- Klein RJ, Zeiss C, Chew EY, et al. Complement factor H polymorphism in age-related macular degeneration. Science. 2005;308(5720):385-389.
- Fritsche LG, Igl W, Bailey JN, et al. A large genome-wide association study of age-related macular degeneration highlights contributions of rare and common variants. Nat Genet. 2016;48(2):134-143.
- Klein ML, Francis PJ, Rosner B, et al. CFH and LOC387715/ARMS2 genotypes and treatment with antioxidants and zinc for age-related macular degeneration. Ophthalmology. 2008;115(6):1019-1025.
- Awh CC, Lane AM, Hawken S, Zanke B, Kim IK. CFH and ARMS2 genetic polymorphisms predict response to antioxidants and zinc in patients with age-related macular degeneration. Ophthalmology. 2013;120(11):2317-2323.
- Chew EY, Klein ML, Clemons TE, et al. No clinically significant association between CFH and ARMS2 genotypes and response to nutritional supplements: AREDS report number 38. Ophthalmology. 2014;121(11):2173-2180.
- Assel MJ, Li F, Wang Y, Allen AS, Baggerly KA, Vickers AJ. Genetic polymorphisms of CFH and ARMS2 do not predict response to antioxidants and zinc in patients with age-related macular degeneration. Independent statistical evaluations of data from the Age-Related Eye Disease Study. Ophthalmology. 2018;125(3):391-397.
- Stone EM, Aldave AJ, Drack AV, et al. Recommendations for genetic testing of inherited eye diseases: report of the American Academy of Ophthalmology task force on genetic testing. Ophthalmology. 2012;119(11):2408-2410.
- Teutsch SM, McCoy MA, Woodbury RB, Welp A, eds. Making eye health a population health imperative. The National Acadamies Press; Washington, DC. Available at https://www.nap.edu/read/23471/chapter/1 .