







High myopia (HM) is a clinical condition characterized by a progressive axial elongation of the eye, associated in 48% of cases with a posterior staphyloma (PS), which leads to an increased risk of specific tractional diseases involving the macular region. Currently, different surgical procedures have been proposed to treat these HM patients, and one of them is the macular buckling (MB) technique.
Although it was used for the first time by Schepens et al in 1957 to treat retinal detachment due to macular hole (MHRD) in HM eyes, and despite that several studies have also been published thereafter with promising results, it is only over the last 2 decades that this procedure has started to regain ground among vitreoretinal surgeons.1
The common belief that MHRD is a challenging surgical technique that requires a longer learning curve than pars plana vitrectomy (PPV), the potential damage to the surrounding ocular structures (ie, vortex veins and short ciliary vessels, the optic nerve, and extraocular muscles), and the risk of drainage-related hemorrhages due to intraoperative manipulation of the eye have prevented this procedure from becoming more widespread. In addition, the lack of easily commercially available posterior buckles might be another restrictive factor. Therefore, attention was drawn away from the MB technique until the 2000s, when Sasoh et al reported a more than 90% anatomical success rate after MB in HM eyes with MHRD.2 Since then, dozens of articles have been published on this type of surgery, including yearly since 2011.3-21 This new interest might be explained by gradual recognition of the MB as the only way to counteract the pulling effect of the PS typical of HM.
Retina specialists know that excessive axial elongation of the globe and the development of a PS, as may occur in HM eyes, can cause mechanical stretching of the ocular structures, accompanied by thinning of the sclera and choroid, resulting in various retinal degenerative changes.
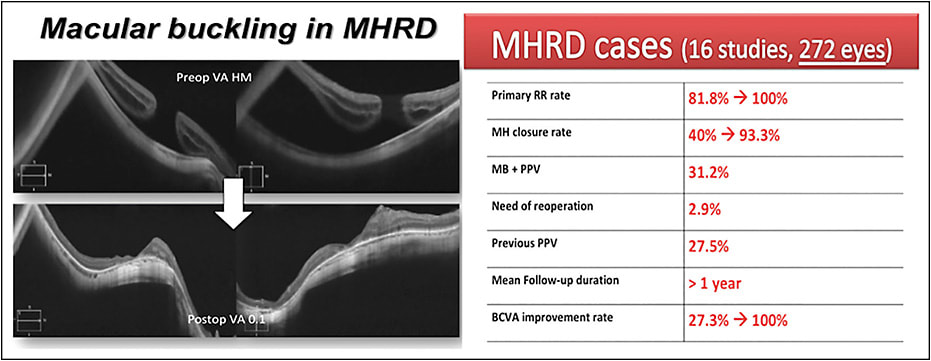
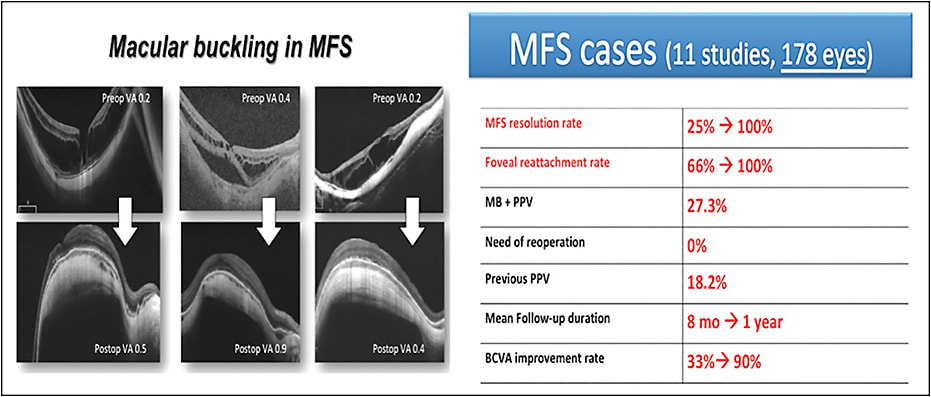
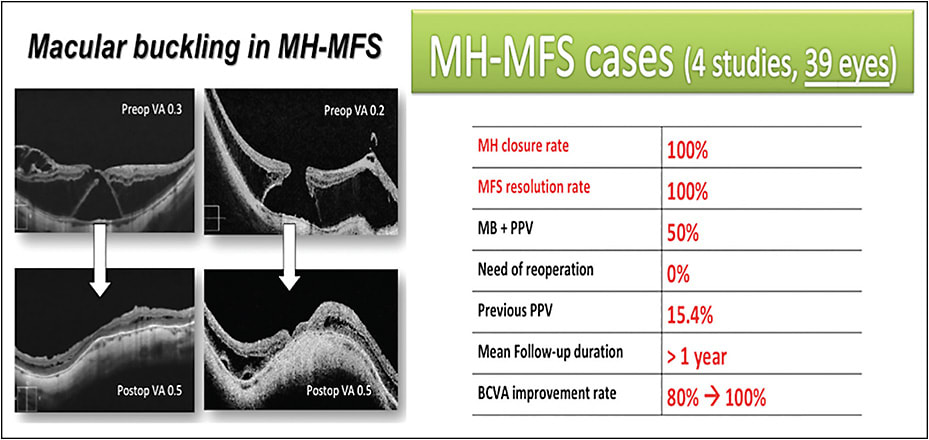
Among other causative factors, including inner traction due the vitreous cortex, premacular structures, internal limiting membranes, and vascular stiffness, these patients may develop serious complications, such as MHRD (Figure 1); myopic foveoschisis (MFS) with or without foveal detachment (FD) (Figure 2); and MFS associated with macular hole (MH) (Figure 3).
Whatever the pathogenic mechanism, these 3 conditions are actually 3 specific vitreoretinal disorders grouped into the term myopic traction maculopathy, which share the presence of a PS as the lowest common denominator.22
Moreover, although they can be considered 3 different clinical entities, they may not be completely separated from each other since their natural history shows that they are progressive conditions and that the presence of an MFS seems to represent the most important risk factor for the final stage of MHRD.23-27 Thus, it might sound like an easy equation, that is, “posterior staphyloma = myopic traction maculopathy = macular buckling,” but the truth is unfortunately more complicated.
Not all PS are able to induce these retinal diseases. Specifically, in “deeper” PS, which are often limited to the macular region, centripetal vector forces exerted toward the center of the globe are greater than in eyes with a flatter PS. As a consequence, because the relatively inelastic inner retina tends to resist the anteroposterior traction exerted by the staphyloma, the retina can split, leading initially to an MFS and finally to a posterior retinal detachment with or without MH formation.
Considering all of these points, although the transvitreal approach can help to eliminate some important types of traction, it cannot do anything to alleviate the progressive scleral ectasia of the myopic staphyloma, and this is where the MB technique comes in (Figure 4). Of course, there is nothing that prevents vitreoretinal surgeons from performing MB and PPV in a “1-step surgery” or limiting this combined approach in recurrent or persistent cases, and it is likely that it is even more true that there is no more evidence-based science for any surgeon than his or her own personal experience.
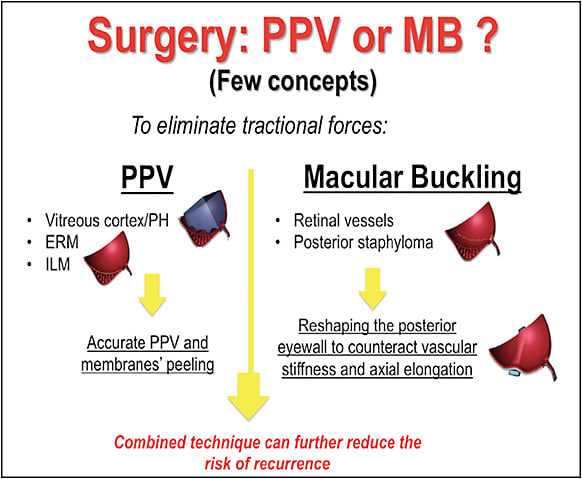
However, adding MB to PPV can first counteract and further invert the inner forces of the stretched retinal vessels in the area of the staphyloma and release the tangential tractional forces that cannot be reduced with PPV alone. Second, with the combined approach, there is no need for trans-scleral drainage, which avoids possible complications such as perforation of the globe or choroidal detachment with choroidal effusion in some cases.28-31
Nevertheless, in making our surgical choices, we cannot entirely ignore what has been published in the literature in terms of anatomical success rates, visual improvement, and complication rates.
Recently, we conducted a literature review of the MB technique, including all of the published studies in which this procedure has been applied from 2000 to 2016, resulting in 31 papers and 489 eyes.32 When analyzing both the anatomical and functional results in the 3 different retinal conditions (MHRD, MFS, and MH-MFS), we also focused our attention on the aforementioned queries, concluding that the posterior episcleral approach is a safe and effective procedure to treat HM eyes affected by myopic traction maculopathy.32
CASES OF RETINAL DETACHMENT DUE TO MACULAR HOLE
As shown in Figure 1, among 272 eyes affected by MHRD that were treated with MB, the primary retinal reattachment and MH closure rates ranged from 81.8% to 100% and from 40% to 93.3%, respectively.6,7 Only 2.9% of these patients underwent a second surgery due to persistent MHRD, while previous unsuccessful PPV (1 to 3) was performed in almost one-third of patients. Overall, slightly more than one-third of patients underwent a combined MB and PPV.
All of these findings suggest that, first, if vitreous surgery is planned alone, closing the MH is important to avoid retinal redetachment in these eyes and, second, the retina does not redetach in cases of persistent MH supported by posterior buckles. Only 3 studies comparing PPV and MB have been published, showing that these anatomical rates are generally lower with PPV than MB.14,28,30
Thus, in answering the first query above, the reply might be ”Yes, it works.” Moreover, it seems that it works even better in eyes with an axial length greater than 30 mm. Specifically, based on our review’s data, the retina reattaches in 100% of cases, and the MH closure rate ranges from 40% to 100% in these longer eyes.4,5,9-11,13,14 In contrast, these rates are rarely obtained with PPV. We would like to be able to say this when we dare to affirm that MB seems to achieve better anatomical success rates than vitreous surgery.
Regarding functional results, 27.3% to 100% of patients included in this group experienced such a visual improvement. It should be noted that the rate was less than 50% in 2 of 16 studies and was greater than this value in 14, reaching 100% in 6 case series.
MYOPIC FOVEOSCHISIS CASES
Different pattern of MFS may exist, and although PPV with conventional internal limiting membrane (ILM) peeling has demonstrated good results in isolated MFS, it has been also been reported that this procedure may induce postoperative MH in 27% of cases, which with time may evolve to MHRD in some cases.27,33
How can we avoid this risk? Because we now live in the OCT age, deciding on the best surgical approach may also depend on the information observed from OCT images and correctly using these data. For example, if a thin “roof” is detected on OCT scans at the level of foveal detachment in MFS cases, 2 different surgical solutions are possible. The first might be the episcleral approach, as we recently reported.
Indeed, in our review of 178 eyes affected by MFS with or without foveal detachment and treated with MB (Figure 2), foveoschisis completely resolved in 100% of patients in 5 of the 11 studies, and the resolution rate ranged from 25% to 94.9% in the others.4,10,14-17,34,35 The final foveal reattachment rate was 100% in 8 case series.
Regarding the surgical technique, MB was associated with PPV with or without ILM peeling in approximately 27% of cases. Overall, while 18.2% of patients had undergone previous unsuccessful PPV, there was no need for reoperation after MB, and final BCVA improved in 33.3% to 90% of cases.
The second option might include PPV with the “foveal sparing” technique, in which the ILM removal is limited to the macular region without crossing the fovea, thus likely eliminating the most important tangential traction, relaxing the retina, and eliminating the risk of inducing a full-thickness MH.36
Despite the excellent results that we have obtained with the episcleral approach in these cases, we cannot forget that, apart from the technical difficulties, MB induces a hyperopic shift that cannot be easily tolerated in some patients with good bilateral vision.32 Thus, our current choice is to perform PPV with ILM removal sparing the foveal area in such patients, observing no risk of iatrogenic MH, complete foveal reattachment, and resolution of foveoschisis. However, to date, the types of MFS suitable for PPV or MB remain unclear, and further studies are necessary.
Whatever the surgery, one might ask, “When should we operate on these patients?” Some authors have suggested that surgical and functional benefits are greater in patients with foveal detachment than in those with isolated MFS.37 As users of OCT technology, we believe that, if tomographic images document real progression of the disease, then the patient should be closely monitored to plan the surgical treatment in cases of a rapid visual impairment. This strategy should also prevent the possible unfortunate final stage of MHRD. In other words, the ideal timing for surgery should be soon enough to be both therapeutic and preventive.
MACULAR HOLE-MYOPIC FOVEOSCHISIS CASES
Two different types of myopic MH can exist, based on whether or not it is associated with concomitant foveoschisis. In general, the prognosis is usually better in cases involving only MH without foveoschisis than in cases with MH and associated foveoschisis. As for all HM eyes, an axial length greater than 30 mm also seems to represent a negative factor preventing surgical success with PPV in these cases.38
Thus, although the treatment of MH without foveoschisis can be similar to that used for nonmyopic cases, including PPV, ILM peeling, and intraocular tamponade with gas or silicone oil, this approach seems insufficient in cases of MH-MFS for which MB should be considered. Curiously, among all 489 of the eyes treated with MB, only 39 belonged to this subgroup. The reason could be the natural clinical evolution of this retinal condition: HM eyes affected by MH with concomitant MFS seem to quickly progress to MHRD.
Regarding both anatomical and functional outcomes, excellent results have been obtained with MB in these cases. Specifically, MFS resolution and MH closure were achieved in 100% of patients with no need for reoperation, and vision improved in 80% to 100% of the eyes. Previous unsuccessful vitrectomy had been performed in 15% of patients, who thus required a second surgical approach with posterior buckles.32
TYPES OF BUCKLES, TECHNIQUES, AND COMPLICATIONS
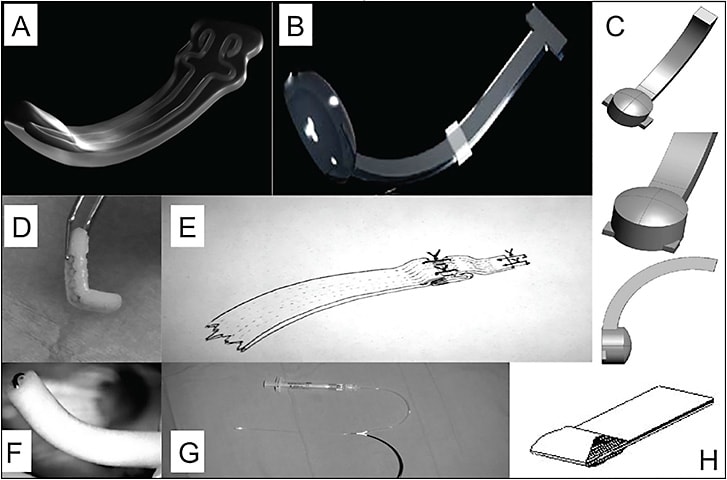
New posterior buckles of different shapes and materials have been proposed. To date, there are only 3 commercially available macular exoplants in Europe: the AJL Macular Buckle (AJL Ophthalmic); the T-shaped Buckle (FCI); and the Adjustable Macular Buckle (Micromed). Despite the Japanese Ando plombe (Ondeko Corporation) having been used in the Asian population, we are unsure of its commercial availability. Moreover, to our knowledge, a macular exoplant does not commercially exist in the United States.
Thus, due to these problems, most of the MBs indicated in Figure 5, which have been used in several published studies, are actually “homemade.”32,39,40 Independent of the material, an additional stainless steel or titanium wire can also be used, allowing the MB to be bent as needed until the desired shape is obtained (T shape or L shape) for correct indentation. In addition, a 29-gauge chandelier light may be inserted into the indenting head of the MB for optimal positioning, when needed.2-5
Several surgical techniques have been proposed in the last few years. The main differences among them include rectus muscle involvement, the need for posterior scleral suture while placing the buckle, and trans-scleral posterior drainage.
Concerning possible complications, it is recognized that HM patients have a greater risk of developing choroidal hemorrhage due to their lower scleral rigidity. The manipulation of the sclera and the placing of posterior sutures could cause this complication.
Moreover, these eyes are often characterized by progressive scleral thinning, which may increase the risk of eye perforation, forcing the surgeon in some cases to look for a better location to place the initial mattress suture. For the same reason, in trying to reduce the risk of unintentional hypotony and choroidal effusion in cases of scleral perforation, we suggest applying the first nylon-suture in a closed eye if a combined PPV-MB approach is planned.
All buckles using a nasal-to-nasal approach can induce muscle injury and vortex vein damage, which can lead to choroidal detachment in severe cases.18,35 However, there are other techniques that are no less effective but more complex to pursue, such as implantation of a silicone band 6 mm in width from the inferonasal quadrant to superonasal quadrant that passes beneath the macular area. Using this type of MB, it is very important to place the silicone band behind the insertion of the tendon of the inferior oblique muscle and to position it behind where the inferior temporal vortex veins perforate the sclera. This maneuver requires special attention because it can compress the exit of this vortex vein and cause a choroidal detachment, especially in the inferior quadrants.
With posterior buckles to be positioned in one quadrant (ie, Ando plombe, AJL Macular Buckle, L-shaped buckles), we should be cautious with the superotemporal vortex vein, which is located at the insertion of the tendon of the superior oblique muscle. Because these buckles must be positioned in the center of the superotemporal quadrant, they are less likely to injure this vein.
It is undebatable that some techniques may be associated with a higher risk of complications than others and might be more challenging because of technical difficulties when placing the exoplant.41 Furthermore, some buckles may induce excessive compression under the choroidal vessels and cause retinal pigment epithelium (RPE) changes and serous foveal detachment.42
Despite these technical difficulties, we found that MB has shown a generally low rate of complications in reviewing all 31 of the published studies. Specifically, the most common were RPE changes (>2.4%), MB removal (2%), malpositioning requiring surgery (1.8%), and choroidal effusion (1.4%). Scleral perforation, which is commonly considered one of the main risks because of the scleromalacia typical of these eyes, was described in only 7 of 489 cases (1.4%).
Regarding the effect on the RPE of posterior buckles, we have observed more postoperative RPE changes after using the Ando plombe, probably due to the overly square indenting head typical of this exoplant. Conversely, a better status of the RPE is observed when using different plombes with a rounded platform.
FUTURE PERSPECTIVES
Today, our clinical practice cannot be separated from OCT technology, especially in these HM eyes in which biomicroscopy during a normal fundus examination risks underestimating the presence of some clinical disorders due to the lack of contrast in cases of extensive chorioretinal atrophy. Tomographic scans enable detection of any foveal defects in these eyes, thus avoiding the risk of losing data. Tomography is strongly suggested pre- and postoperatively. However, because we live in the era of “new OCT instrumentation,” special attention must be paid to the development of intraoperative OCT (iOCT), the use of which is not specific to HM patients. Real-time OCT imaging can facilitate the placement of any posterior exoplant under the macular region in terms of both height and position, allowing for ideal buckling. Indeed, it is possible that some MHs remained open despite retinal reattachment, likely because of excessive or insufficient posterior indentation. Moreover, iOCT can improve identification and removal of premacular traction during PPV, and direct visualization of a thin or thick roof in MFS, visualized by iOCT, could guide vitreoretinal surgeons in their choices of whether and how to perform ILM peeling to minimize the risk of iatrogenic MH.
One of the most innovative advances in the MB technique currently might be the suprachoroidal injection of long-acting hyaluronic acid.10 The main advantage of this strategy seems to be the ability to indent the macular area without directly compressing the posterior vessels, thereby reducing the risk of secondary RPE atrophy. In addition to the challenge of correctly administering the injection and delivering a sufficient volume when addressing both deep or combined PS, another factor to considered is the temporary effect of hyaluronic acid, which renders the indentation reversible after approximately 1 year. Nevertheless, some studies have shown that when the MB is removed in MHRD eyes, the MH remains closed and the retina attached. In cases of extrusion, diplopia, or infection, however, any MB can also be removed, if necessary, which seems not to influence anatomical outcomes even several years later. This suggests that permanent indentation might not be necessary.
CONCLUSION
Although several approaches and posterior exoplants may be used for MB surgery, all of them share the common purpose of reshaping the posterior eyewall to reduce retinal traction. As far as we know, this is actually the only surgical technique able to mechanically counteract the traction exerted by the PS, which leads to myopic tractional maculopathy.
Complete resolution of the foveoschisis, retinal reattachment, and concomitant MH closure seem to be achieved more frequently with MB than with PPV. This difference appears to be even more true when considering those patients with greater axial length, in whom MH closure is rarely obtained with vitreous surgery. Indeed, a deep PS and a persistent MH after PPV should be considered the 2 main risk factors for retinal detachment in HM eyes. As a consequence, when MB is applied, whether alone or combined with PPV, multiple surgeries are less commonly required. RP
REFERENCES
- Schepens CL, Okamura ID, Brockhurst RJ. The scleral buckling procedure. I. Surgical technique and management. AMA Arch Ophthalmol. 1957;58(6):797-811.
- Sasoh M, Yoshida S, Ito Y, et al. Macular buckling for retinal detachment due to macular hole in highly myopic eyes with posterior staphyloma. Retina. 2000;20(5):445-449.
- Mateo C, Dutra Medeiros M, Alkabes M, et al. Illuminated Ando plombe for optimal positioning in highly myopic eyes with vitreoretinal diseases secondary to posterior staphyloma. JAMA Ophthalmol. 2013;131(10):1359-1362.
- Parolini B, Frisina R, Pinackatt S, et al. Indications and results of a new L-shaped macular buckle to support a posterior staphyloma in high myopia. Retina. 2015;35(12):2469-2482.
- Forlini M, Szkaradek M, Rejdak R, et al. Modification of adjustable macular buckling with 29-G chandelier light for optimal positioning in highly myopic eyes with macular hole. Retin Cases Brief Rep. 2017;11(3):249-254.
- Devin F, Tsui I, Morin B, et al. T-shaped scleral buckle for macular detachments in high myopes. Retina. 2011;31(1):177-180.
- Tian J, Tang LS, Guo XJ, Luo YH. Episcleral macular buckling for posterior retinal detachment in silicone oil filled eyes associated with myopic macular hole. Int J Ophthalmol. 2013;6(2):165-168.
- Alkabes M, Burés-Jelstrup A, Salinas C, et al. Macular buckling for previously untreated and recurrent retinal detachment due to high myopic macular hole: a 12-month comparative study. Graefes Arch Clin Exp Ophthalmol. 2014;252(4):571-581.
- Mortada HA. A novel episcleral macular buckling: wire-strengthened sponge exoplant for recurrent macular hole and retinal detachment in high myopic eyes. Med Hypothesis Discov Innov Ophthalmol. 2013;2(1):14-19.
- El Rayes EN. Supra choroidal buckling in managing myopic vitreoretinal interface disorders: 1-year data. Retina. 2014;34(1):129-135.
- Mura M, Iannetta D, Buschini E, de Smet MD. T-shaped macular buckling combined with 25G pars plana vitrectomy for macular hole, macular schisis, and macular detachment in highly myopic eyes. Br J Ophthalmol. 2017;101(3):383-388.
- Siam AL, El Maamoun TA, Ali MH. Macular buckling for myopic macular hole retinal detachment: a new approach. Retina. 2012;32(4):748-753.
- Bedda AM, Abdel Hadi AM, Abd Al Shafy MS. A comparative study between vitrectomy with internal tamponade and a new modified fiber optic illuminated Ando plombe for cases of macular hole retinal detachment in myopic eyes. J Ophthalmol. 2015;2015:841925.
- Qi Y, Duan AL, You QS, et al. Posterior scleral reinforcement and vitrectomy for myopic foveoschisis in extreme myopia. Retina. 2015;35(2):351-357.
- Li XJ, Yang XP, Li QM, et al. Posterior scleral reinforcement combined with vitrectomy for myopic foveoschisis. Int J Ophthalmol. 2016;9(2):258-261.
- Mateo C, Gómez-Resa MV, Burés-Jelstrup A, Alkabes M. Surgical outcomes of macular buckling techniques for macular retinoschisis in highly myopic eyes. Saudi J Ophthalmol. 2013;27(4):235-239.
- Ji X, Wang J, Zhang J, et al. The effect of posterior scleral reinforcement for high myopia macular splitting. J Int Med Res. 2011;39(2):662-666.
- Liu B, Ma W, Li Y, et al. Macular buckling using a three-armed silicone capsule for foveoschisis associated with high myopia. Retina. 2016;36(10):1919-1926.
- Zhu Z, Ji X, Zhang J, Ke G. Posterior scleral reinforcement in the treatment of macular retinoschisis in highly myopic patients. Clin Exp Ophthalmol. 2009;37(7):660-663.
- Burés-Jelstrup A, Alkabes M, Gómez-Resa M, et al. Visual and anatomical outcome after macular buckling for macular hole with associated foveoschisis in highly myopic eyes. Br J Ophthalmol. 2014;98(1):104-109.
- Cacciamani A, Lazzeri S, Rossi T, et al. Adjustable macular buckling for full-thickness macular hole with foveoschisis in highly myopic eyes: long-term anatomical and functional results. Retina. 2016;36(4):709-716.
- Panozzo G, Mercanti A. Optical coherence tomography findings in myopic traction maculopathy. Arch Ophthalmol. 2004;122(10):1455-1460.
- Gaucher D, Haouchine B, Tadayoni R, et al. Long-term follow-up of high myopic foveoschisis: natural course and surgical outcome. Am J Ophthalmol. 2007;143:455-462.
- Shimada N, Ohno-Matsui K, Baba T, et al. Natural course of macular retinoschisis in highly myopic eyes without macular hole or retinal detachment. Am J Ophthalmol. 2006;142: 497-500.
- Sun CB, Liu Z, Xue AQ, Yao K. Natural evolution from macular retinoschisis to full-thickness macular hole in highly myopic eyes. Eye (Lond). 2010;24(12):1787-1791.
- Jo Y, Ikuno Y, Nishida K. Retinoschisis: a predictive factor in vitrectomy for macular holes without retinal detachment in highly myopic eyes. Br J Ophthalmol. 2012;96(2):197-200.
- Ikuno Y. Tano Y. Vitrectomy for macular holes associated with myopic foveoschisis. Am J Ophthalmol. 2006;141(4):774-776.
- Ripandelli G, Coppé AM, Fedeli R, Parisi V, D’Amico DJ, Stirpe M. Evaluation of primary surgical procedures for retinal detachment with macular hole in highly myopic eyes: a randomized comparison of vitrectomy versus posterior episcleral bucking surgery. Ophthalmology. 2001;108(12):2258-2264.
- Ripandelli G, Parisi V, Friberg TR, Coppé AM, Scassa C, Stirpe M. Retinal detachment associated with macular hole in high myopia: using the vitreous anatomy to optimize the surgical approach. Ophthalmology. 2004;111(4):726-731.
- Ando F, Ohba N, Touura K, Hirose H. Anatomical and visual outcomes after episcleral macular buckling compared with those after pars plana vitrectomy for retinal detachment caused by macular hole in highly myopic eyes. Retina. 2007(1);27:37-44.
- Siam AL, El Maamoun TA, Ali MH. Macular buckling for myopic macular hole retinal detachment: a new approach. Retina. 2012;32(4):748-753.
- Alkabes M, Mateo C. Macular buckle technique in myopic traction maculopathy: a 16-year review of the literature and a comparison with vitreous surgery. Graefes Arch Clin Exp Ophthalmol. 2018;256(5):863-877.
- Gaucher D, Haouchine B, Tadayoni R, et al. Long-term follow-up of high myopic foveoschisis: natural course and surgical outcome. Am J Ophthalmol. 2007;143(3):455-462.
- Baba T, Tanaka S, Maesawa A, et al. Scleral buckling with macular plombe for eyes with myopic macular retinoschisis and retinal detachment without macular hole. Am J Ophthalmol. 2006;142(3):483-487.
- Mateo C, Burés-Jelstrup A, Navarro R, Corcóstegui B. Macular buckling for eyes with myopic foveoschisis secondary to posterior staphyloma. Retina. 2012;32(6):1121-1128.
- Shimada N, Sugamoto Y, Ogawa M, et al. Fovea-sparing internal limiting membrane peeling for myopic traction maculopathy. Am J Ophthalmol. 2012;154(4):693-701.
- Ikuno Y, Sayanagi K, Soga K, et al. Foveal anatomical status and surgical results in vitrectomy for myopic foveoschisis. Jpn J Ophthalmol. 2008;52(4):269-276.
- Suda K, Hangai M, Yoshimura N. Axial length and outcomes of macular hole surgery assessed by spectral-domain optical coherence tomography. Am J Ophthalmol. 2011;151(1):118-127.
- Pradeep S, Vinay Kumar S. Macular buckle in myopia. Sci J Med Vis Res Found. 2015;33:71-74.
- Rosales Meneses JL. Macular buckle: indication and limitations. EC Ophthalmol. 2012;6(5):141-144.
- Alkabes M, Quijano C, Mateo C. Macular buckling technique in high myopia. In: Patelli F, Rizzo S (eds). Management of Complicated Vitreoretinal Diseases. New York, NY; Springer; 2015:1-20.
- Mateo C, Burés-Jelstrup A. Macular buckling with Ando plombe may increase choroidal thickness and mimic serous retinal detachment seen in the tilted disk syndrome. Retin Cases Brief Rep. 2016;10(4):327-330.