







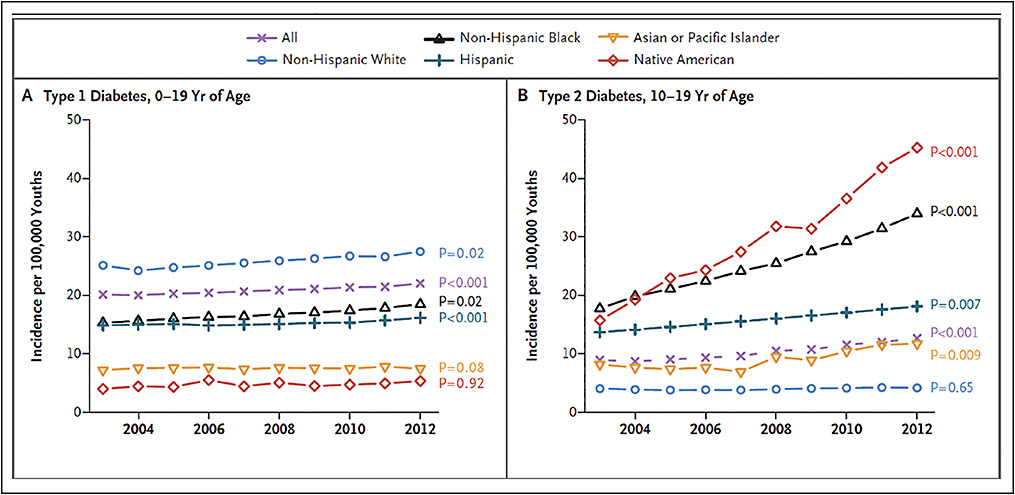
The incidence of type 1 diabetes mellitus (T1DM) and type 2 diabetes mellitus (T2DM) is rising among youth in the United States and around the world (Figure 1).1-3 In the past, children and adolescents were diagnosed most commonly with T1DM, but currently, T2DM accounts for approximately half of all new cases of DM among adolescents worldwide.4 This correlates with the rise in childhood obesity.4 An increase in the incidence and prevalence of diabetes has been accompanied by an increase in diabetic retinopathy (DR) in youths and adults. Diabetic retinopathy is currently the most common cause of blindness in adults in the United States.5
HOW COMMON IS DR IN OUR YOUTH?
The prevalence of DR among young children is low, but the risk of developing microvascular complications increases during the teenage years. Documented rates of DR among children and adolescents vary significantly. In a recent publication in JAMA, Dabelea et al reported the association of T1DM vs T2DM diagnosed during childhood and adolescence with complications during teenage years and young adulthood in 2018 participants across the United States from 2002 through 2015; approximately 5% of participants with T1DM and 9.1% of those with T2DM had developed DR.6 Interestingly, the odds ratio for DR among patients with T2DM vs T1DM remained significant when measures of obesity were added to the logistic regression models.6
A pilot study for the US SEARCH for Diabetes in Youth cohort reported that among 265 individuals with DM diagnosed prior to 20 years of age, 17% with T1DM and 42% with T2DM developed DR detectable on fundus photography over a median follow-up of 6.8 years.7 In a Canadian cohort of children and adolescents, 13.8% of 1,011 youths with T1DM and 11.7% of 342 youths with T2DM had developed DR after 4.4 and 6.7 years, respectively.8 In the TODAY clinical trial, among 517 participants with T2DM in the United States, the prevalence of DR after a mean DM duration of 4.9 years was 13.7%.9 In a cross-sectional study of 482 Australian children and adolescents with T1DM, Keel et al observed a DR prevalence of 2.3%.10
Earlier this year, the results of the largest study to evaluate the incidence and risk factors for developing DR among youths with T1DM and T2DM throughout the United States were published. In this study of 2,240 youths with newly diagnosed T1DM and 1,768 with newly diagnosed T2DM from a large US managed care network, Wang et al reported that 20.1% of youths with T1DM and 7.2% with T2DM with a median of 3.2 and 3.1 years of follow-up, respectively, received a diagnosis of DR. Median age at initial DR diagnosis was 14.2 years for T1DM and 20.4 years for T2DM. Key findings from this study include that for each year older a child was at initial DM diagnosis, the risk for developing DR increased among individuals with T1DM, and every 1-point increase in HbA1c increased the hazard of developing DR by 20% to 30% among those with T1DM or T2DM.11
RISK FACTORS
While it has been well established that delay in DM diagnosis and poor glycemic control increase the risk of development of DR, there are other reported risk factors for DR development in diabetic youths, including male gender and lower household net worth in type 2 diabetics.11 Higher serum creatinine, older age, higher blood pressure, higher body mass index, lower HDL cholesterol, and longer duration of DM (especially in prepubertal years) have been associated with development of DR in children with T1DM.10
NATURE OF DR IN YOUTH-ONSET DM
Of the 578 (14.4%) patients with DR in the study reported by Wang et al, 13 youths were diagnosed with proliferative DR (PDR) and 12 of those had T1DM. The age at diagnosis of PDR ranged from 6 years to 31 years. Diabetic macular edema was diagnosed in 5 persons, all with T1DM, at ages ranging from 15 years to 29 years. Interestingly, none of the patients with PDR and/or DME underwent panretinal photocoagulation, focal laser, or intravitreal injection. The authors reason that this could be attributed to conservative management, treatment refusal, or perhaps incorrect billing or diagnosis code.11
Other studies also support that DR requiring laser treatment rarely occurs within the first 10 years of a child’s diagnosis with T1DM, but that after decades with the disease, the proportion of patients with T1DM requiring laser climbs to >60%.12-14 Detecting diabetes and DR as early as possible is imperative in preventing potentially devastating vision loss that can ensue in the teenage years and beyond.
CURRENT SCREENING GUIDELINES
Current American Academy of Ophthalmology (AAO) screening guidelines for DR recommend initial screening for DR at the time of DM diagnosis for individuals with T2DM and, for individuals with T1DM, at 5 years after T1DM onset.15,16 The American Diabetes Association recommends initial screening for DR 3-5 years after T1DM onset for individuals ≥10 years of age and, for youths with T2DM, recommends screening for DR at the time of T2DM diagnosis.17 The American Academy of Pediatrics recommends initial screening for DR 3 years to 5 years after T1DM onset for individuals ≥9 years of age.18
In analyzing their cohort of nearly 4,000 patients, Wang et al found that waiting 3 years to 5 years after diagnosis of T1DM to screen for DR would have delayed the diagnosis of DR in 18% of patients by 3 years and 25% by 5 years.11
The entirety of data presented in the aforementioned studies support early screening (perhaps at diagnosis) not only for youth diagnosed with T2DM but also for children diagnosed with T1DM. Early identification of DM and DR offers the best opportunity for preventing vision loss.
INADEQUATE SCREENING UNDER CURRENT GUIDELINES
Earlier DR screening for our youth with DM is a step in the right direction, but the fact that less than 50% of patients with DM meet current screening recommendations19 means there is poor compliance with even the current guidelines, and this represents another barrier to our youth receiving the care they need to optimize the prevention of vision loss.
Wang et al recently published results of their investigation of ophthalmic screening patterns among youths with diabetes enrolled in a large US managed care network.20 This retrospective, longitudinal cohort study examined youths 21 years or younger with newly diagnosed diabetes from January 1, 2001 through December 31, 2014. Among 5,453 youths with T1DM and 7,233 youths with T2DM, only 64.9% of patients with T1DM and 42.4% of patients with T2DM had undergone an eye examination by 6 years after initial diabetes diagnosis. African American youths and Latino youths were less likely to have undergone retinal examination as were youths from less affluent families.20
Other barriers to DR screening include lack of insurance, delayed referrals from primary care physicians, lack of patient or family awareness regarding the importance of regular retinal examinations, and the need for parents or other caregivers to take time away from work to take youths to their appointments for retinal evaluation. Additionally, among minorities, language, cultural, and educational barriers may contribute.21
COST-CONSCIOUS STRATEGIES TO IMPROVE SCREENING
Telemedicine
Retinal telescreening in primary care or endocrinology offices with remote expert interpretation could be an important strategy to boost DR screening rates. Several recent studies have proven the usefulness of this strategy, including a study by Tapley et al, whose group screened 236 youths with T1DM or T2DM in a pediatric endocrinology clinic. Mean duration since diabetes diagnosis was 5.5 years. More than 97% of the images were gradable. DR was detected in 3.8% of participants and 9.1% of those were visually impaired. Sixty-six percent of individuals screened reported receiving an eye examination within the previous year.22
The impact of onsite screening with a nonmydriatic digital fundus camera for DR at a diabetes outpatient clinic was investigated by Roser et al in a cross-sectional study that included 502 adult patients, including 112 with T1DM and 390 with T2DM. For T1DM and T2DM patients overall, the prevalence of DR was 25% and the incidence of DR was 6.4%. Approximately 25% of all DR cases were newly diagnosed.23
Telemedicine offers several advantages over the current paradigm. Considering that the incidence and prevalence of diabetes is on the rise, the current healthcare system will likely be unable to accommodate the growing number of patients who will need to be screened in clinic for DR. Also, telemedicine has the potential to increase DR surveillance rates since patients could undergo DR screening at the time of their primary care evaluation rather than having to make (and keep) a separate appointment for a retinal evaluation. Ophthalmologists, in turn, would then be able to see more diabetic patients who truly need treatment rather than diabetic patients with normal retinal exams. Targeted referrals would be more cost-effective than having subspecialists examine all diabetic patients. Additionally, telemedicine would allow screening to reach patients in more rural areas, which can foster earlier diagnosis and referral for treatment.21
Numerous technological advancements are being evaluated that could facilitate retinal telescreening nonmydriatic fundus cameras with better resolution and improved portability. Automated analysis of retinal images using artificial intelligence is also under investigation. Gulshan et al applied deep learning, a family of computational methods that allow an algorithm to program itself by learning from a large set of examples, to create an algorithm for automated detection of DR and DME displayed in retinal fundus photographs. In an evaluation of retinal fundus photographs of adults with DM, the algorithm based on deep learning demonstrated high sensitivity and specificity for detecting DR. For example, in the EyePACS-1 dataset that consisted of 9,963 images from 4,997 patients, the sensitivity for detecting DR was 90.3% and the specificity was 98.1%. For detecting DME, the sensitivity was 90.8% and the specificity 98.7%.24
Individualized, Evidence-Based Screening
The Diabetes Control and Complications Trial (DCCT) and the Epidemiology of Diabetes Interventions and Complications (EDIC) Research Group recently formulated a rational, data-driven strategy to screen for DR in patients with T1DM with an individualized, cost-conscious method. Using Markov models based on 24,000 ophthalmic assessments with fundus photography performed at intervals of 6 months to 48 months during almost 30 years of follow-up, the group formulated a screening schedule based on controlling the probabilities of progression to advanced DR from lesser states to within acceptable limits.
These data suggest that a practical, evidence-based schedule for time to next examination is 4 years for an individual with no retinopathy, 3 years for mild nonproliferative DR (NPDR), 6 months for moderate NPDR, and 3 months for severe NPDR. The authors suggest that this screening schedule would provide a shorter time during which PDR or DME would go undetected and would require fewer examinations compared to the at least annual screening schedule recommended by the AAO.25,26
SUMMARY
Diabetic retinopathy is a growing global health crisis that has potentially devastating lifetime consequences for young diabetics. The first step in reducing vision loss is early detection of DR. Mounting evidence supports earlier DR screening and increased screening rates. Fostering collaboration between retina specialists and primary care physicians/endocrinologists may lead to efficient, cost-conscious, and quality eye health care for diabetic patients. RP
REFERENCES
- Lawrence JM, Imperatore G, Pettit DJ, et al. Incidence of diabetes in United States youth by diabetes type, race/ethnicity, and age, 2008-2009. Diabetes. 2014;63(Suppl 1):A407.
- Green A, Patterson CC; EURODIAB TIGER Study Group. Europe and iabetes. Trends in the incidence of childhood-onset diabetes in Europe 1989-1998. Diabetologia. 2001;44:B3-B8.
- Lin WH, Wang MC, Wang WM, et al. Incidence of and mortality from type I diabetes in Taiwan from 1999 through 2010. A nationwide cohort study. PLoS One. 2014;9(1):e86172.
- Pinhas-Hamiel O, Zeitler P. The global spread of type 2 diabetes mellitus in children and adolescents. J Pediatr. 2005;146(5):693-700.
- Centers of Disease Control and Prevention. National diabetes fact sheet, 2011: national estimates and general information on diabetes and prediabetes in the United States. Author: Atlanta, 2011. Available at https://www.cdc.gov/diabetes/pubs/pdf/methods11.pdf .
- Dabelea D, Stafford JM, Mayer-Davis EJ, et al. Association of type 1 diabetes vs type 2 diabetes diagnosed during childhood and adolescence with complications during teenage years and young adulthood. JAMA. 2017;317(8):825-835.
- Mayer-Davis EJ, Davis C, Saadine J, et al. Diabetic retinopathy in the SEARCH for Diabetes in Youth Cohort: a pilot study. Diabet Med. 2012;29:1148-1152.
- Dart AB, Martens PJ, Rigatto C, Brownell MD, Dean HJ, Sellers EA.iabet Med. 2004;2(;. 2017J Earlier onset of complications in youth with type 2 diabetes. Diabetes Care. 2014;37(2):436-443.
- TODAY study group. Retinopathy in youth with type 2 diabetes participating in the TODAY clinical trial. Diabetes Care. 2013;36(6):1772-1774.
- Keel S, Itsiopoulos C, Koklanis K, Vukicevic M, Cameron F, Brazionis L. Prevalence and risk factors for diabetic retinopathy in a hospital-based population of Australian children and adolescents with type 1 diabetes. Pediatr Endocrinol Metab. 2016;29(10):1135-1142.
- Wang SY, Andrews CA, Herman WH et al. Incidence and risk factors for developing diabetic retinopathy among youths with type 1 or type 2 diabetes throughout the United States. Ophthalmology. 2017;124(4):424-430.
- Kyto JP, Harjutsalo V, Forsblom et al; FinnDiane Study Group. Decline in the cumulative incidence of severe diabetic retinopathy in patients with type 1 diabetes. Diabetes Care. 2011;34(9):2005-2007.
- Sano H, Nishimura R, Asao K, et al. Diabetes Epidemiology Research International Study Group. Blindness and laser photocoagulation in patients with childhood onset type 1 diabetes in Japan. Br J Ophthalmol. 2009;93(6):726-730.
- Harvey JN, Allagoa B. The long-term renal and retinal outcome of childhood-onset type 1 diabetes. Diabet Med. 2004;21(1):26-31.
- American Academy of Ophthalmology. Screening for retinopathy in the pediatric patient with diabetes mellitus – reaffirmed 2014. http://www.aao.org/clonical-statement/screening-retinopathy-in-pediatric-patient-with-ty-2 .
- American Academy of Ophthalmology. Diabetic retinopathy PPP-2014. http://www.aao.org/preferred-practice-pattern/diabetic retinopathy-ppp-updated-2015 .
- American Diabetes Association. Diabetic retinopathy. Diabetes Care. 2002;25:s90-s93. Available at http://care.diabetesjournals.org/content/25/suppl_1/s90 .
- Lueder GT, Silverstein J; American Academy of Pediatrics Section on Ophthalmology and Section on Endocrinology. Screening for retinopathy in the pediatric patient with type 1 diabetes mellitus. Pediatrics. 2005;116(1):270-273.
- Lee PP, Feldman ZW, Ostermann J, Brown DS, Sloan FA. Longitudinal rates of annual eye examinations of persons with diabetes and chronic eye diseases. Ophthalmology. 2003;110(10):1952-1959.
- Wang SY, Andrews CA, Gardner TW, et al. Ophthalmic screening patterns among youths with diabetes enrolled in a large US managed care network. JAMA Ophthalmol. 2017;135(5):432-38.
- Garg S. Diabetic retinopathy screening with telemedicine: a potential strategy to engage our youth. JAMA Ophthalmol. 2017;135(5):438-439.
- Tapley JL, McGwin Jr. G, Ashraf AA, et al. Feasibility and efficacy of diabetic retinopathy screening among youth with diabetes in a pediatric endocrinology clinic: a cross-sectional study. Diabetol Metab Syndr. 2015;7:56.
- Roser P, Kalscheuer H, Groener JB, et al. Diabetic retinopathy screening ratio is improved when using a digital, nonmydriatc fundus camera onsite in a diabetes outpatient clinic. J Diabetes Res. 2016. [Epub ahead of print]
- Gulshan V, Peng L, Coram, et al. Development and validation of a deep learning algorithm for detection of diabetic retinopathy in retinal fundus photographs. JAMA. 2016;316(22):2402-2410.
- The DCCT/EDIC Research Group, Nathan DM, Bebu I, et al. Frequency of evidence-based screening for retinopathy in type 1 diabetes. N Eng J Med. 2017;376(16):1507-1516.
- American Academy of Ophthalmology. Diabetic retinopathy PPP - Updated 2016. Available at https://www.aao.org/preferred-practice-pattern/diabetic-retinopathy-ppp-updated-2016 .