







Rapid advances in small-gauge vitrectomy tools and techniques have contributed to efficiency, safety, and ultimately better surgical outcomes.
“It has been a complete revolution, starting with patient comfort to having smaller gauge instrumentation that more precisely matches the pathology,” says Colin A. McCannel, MD, Los Angeles. “If we put a 20-gauge instrument in the eye today, it looks like a stone-age club in terms of its size relative to the problem that we are trying to address. Back in the day, we were using gigantic 20-gauge scissors to cut tiny blood vessels between proliferative membranes and the retina, and we used to accidentally create many more holes than we do now. With today’s smaller gauge vitrectomy systems, the scissors are so short, that it’s difficult to cause any collateral damage.
“Better yet, we don’t need to deploy additional instrumentation in many cases,” Dr. McCannel says. “For example, we can use the vitreous cutter for large portions, if not all, of the dissection in diabetic cases, where the pathologies are complex and sometimes difficult. In addition, we have more control over the fluidics with the modern machines, and certainly the EVA is a good example of that.”
What the EVA Brings to the OR
“The two major features I appreciate about the EVA machine are, number one, the TDC cutter with its high flow rate and high cut rate, minimizing vitreous traction in cases where I do not want vitreous traction, and number two, the fluidics to support that minimization of vitreous traction,” Dr. McCannel says. “With the EVA, I can toggle between vacuum control and flow control so that I can use flow control when I’m getting close to the retina and I don’t want to have sudden tissue jumps into my cutting port causing holes that I didn’t intend to make.”
Brian C. Joondeph, MD, Denver, uses 23-gauge instrumentation for most of his surgeries and 27-gauge in select cases, such as non-clearing vitreous hemorrhage, floaters, and some complex diabetic cases. He appreciates that the TDC cutter and various peripheral tools for the EVA system are available in 23-, 25-, and 27-gauge.
“All of the gauges have their roles, and the good surgeon will know what to use in each situation to get the best outcome,” Dr. Joondeph says. “The EVA trocars allow me to make sutureless incisions regardless of which gauge I use, and we use the DORC high-flow infusion line exclusively on all gauges in our surgery centers.”
When discussing fluidics, Yannek Leiderman, MD, PhD, Chicago, notes the VacuFlow technology of the EVA system comes into play when there is a potential mismatch between outflow and inflow. “One example is when we are performing surgery in an air-filled eye,” Dr. Leiderman says. “The EVA vitrectomy system allows us to precisely match the inflow of air with the outflow of tissue or air, thereby preventing any changes in the size of the compartment.
“Another advantage of small-gauge vitrectomy is the ability to remove tissue using the vitrectomy probe at the retinal surface where we need precise control to preserve underlying retinal tissue, such as in cases of complex diabetic tractional retinal detachments,” Dr. Leiderman says. “I have to emphasize that the experience and preferred tactics of the surgeon are significant in terms of being effective with these types of surgical maneuvers in complex cases, but I and other surgeons are excited about developing new tactics and exploring how to best harness these technologies.”
Asheesh Tewari, MD, Ann Arbor, MI, says the EVA features and functions combined help create a smoothly running operating room.
“Our productivity in the OR has definitely improved,” he says. “The TDC cutter is fast and efficient, and the LED light source allows me to perform bimanual surgery, which also helps improve my efficiency.
“Our actual operative time — from the time I sit down at the microscope and begin the surgery to when I make my final closure and pull the microscope away — has decreased compared with when we were using the older technology,” Dr. Tewari says. “Also, from a safety perspective, the VacuFlow technology minimizes the risk of iatrogenic breaks while shaving vitreous during retinal detachment repair.”
Safe, Powerful Visualization With LEDStar Illumination
- Utilizes light-emitting diode technology with long life span (>10,000 hours)
- Has high power threshold before potential for light toxicity
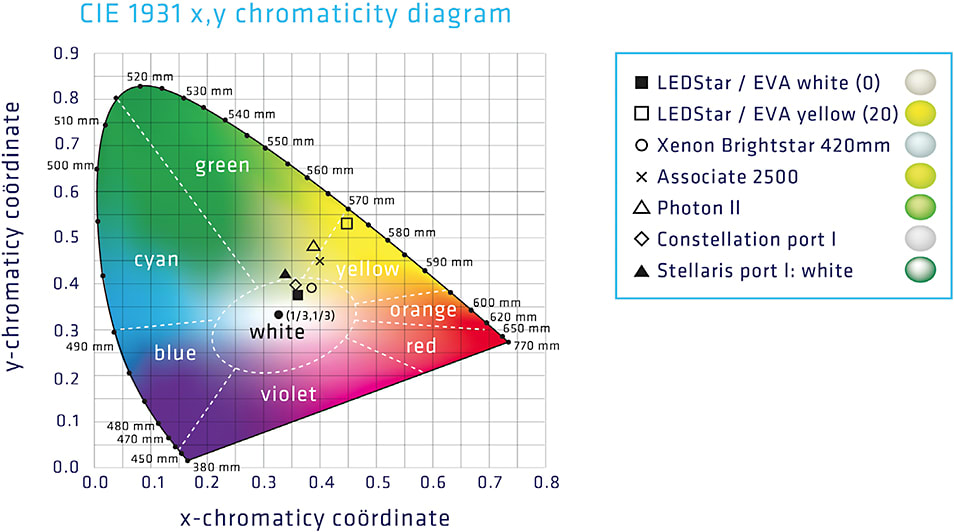
- Allows for color or light temperature adjustments (Figure 1)
- Facilitates bimanual surgical techniques with chandelier illumination*
- Provides up to 40 lumens without degradation of light output
- Delivers more than adequate illumination to differentiate tissues during microincision vitrectomy of all gauges.
*The EVA surgical system has 3 separate LED light ports to accommodate chandelier lighting systems.
Bottom Line: Benefits for Patients
“At the end of the day, the most important deciding factor is how our patients are doing,” Dr. Tewari says. “Are we providing better outcomes? I think the EVA machine helps make surgery safer and more efficient, which are the two goals that we expect from innovation.” ■