







The first part of this series addressed the influence of diagnostic and imaging modalities on the clinical diagnosis and management of pediatric retinal disease, as well as the unique considerations in surgical intervention for children due to anatomic differences between pediatric and adult eyes. This article will review pediatric neovascular retinal disorders, intravitreal anti-VEGF therapy, systemic diseases with retinal manifestations, infectious and noninfectious inflammatory disorders, and intraocular tumors affecting the pediatric population.
PEDIATRIC NEOVASCULAR RETINAL CONDITIONS AND INTRAVITREAL ANTI-VEGF
Vascular endothelial growth factor is an established target for the treatment of neovascular retinal disorders. Intravitreal anti-VEGF medications (bevacizumab, ranibizumab, and aflibercept) have revolutionized the treatment of adult retinal vasoproliferative disorders, such as diabetic retinopathy (DR) and AMD.1,2 Use of intravitreal anti-VEGF medications has also increased in pediatric patients, and it has been used in the treatment of pediatric retinal diseases known to have abnormal neovascularization or vascular defects. These pediatric retinal conditions include Norrie disease,3 familial exudative vitreoretinopathy (FEVR),4,5 Coats disease,6,7 incontinentia pigmenti,8 Eales disease,9 sickle cell retinopathy,10 and retinopathy of prematurity (ROP).11,12
Ru-ik Chee, MD, and Mrinali Patel Gupta, MD, are from the Department of Ophthalmology, Weill Cornell Medical College, New York, New York. Ann-Marie Lobo, MD, and R.V. Paul Chan, MD, are from the Department of Ophthalmology and Visual Sciences, Illinois Eye and Ear Infirmary, University of Illinois at Chicago, Illinois. The authors report no disclosures related to this article. Dr. Chan can be reached at rvpchan@uic.edu.
Intravitreal anti-VEGF medications have been shown to be very effective in promoting regression of neovascularization in many pediatric retinal conditions. However, the safety profile of intravitreal anti-VEGF medications in a pediatric population has not been fully determined. Anti-VEGF therapy has been reported to be associated with complications such as membrane contraction with retinal detachment and delayed-onset retinal detachment.13-17 Secondary delayed retinal detachments are thought to result from the acceleration of the fibrotic component of neovascularization, which may accelerate after intravitreal anti-VEGF therapy. There is concern that intravitreal anti-VEGF therapy can interfere with neurodevelopment and normal development of other organ systems secondary to detectable levels of bevacizumab systemically after intravitreal injection of the drug.18 In the ROP patient, close and extended follow-up is also needed due to the possibility of disease recurrence after primary treatment with anti-VEGF agents.11
Apart from VEGF, Wnt signaling pathways, and Norrin specifically, have been investigated as a potential therapeutic target in retinal vascular diseases associated with retinal ischemia.19 The Wnt signaling pathways are a group of signal transduction pathways that are activated by the binding of a Wnt-protein ligand to a Frizzled family receptor.20 Beta-catenin is involved in the canonical Wnt pathway, and other noncanonical pathways operate independently of beta-catenin.
Norrin is the abnormal protein product of Norrie disease, and it has been shown to activate Wnt signaling in the absence of the Wnt ligand. Norrie disease defects are associated with abnormal vascular and neural tissue development in the eye, ear, and central nervous system. Familial exudative vitreoretinopathy has been associated with mutations resulting in protein products involved in the canonical Wnt and Norrin signaling pathways. The most common of these mutations include Frizzled-4 (FZD4), low-density lipoprotein receptor-related protein 5 (LRP5), tetraspanin-12 (TSPAN12), and Norrin disease protein (NDP) mutations.21-23 LRP5 is the extracellular coreceptor of FZD4, NDP ligand has a strong affinity to FZD4, and the ligand-receptor complex interaction is mediated by TSPAN12.
SYSTEMIC DISEASES WITH RETINAL MANIFESTATIONS
Diabetic retinopathy has been seen in individuals as young as 5 years old.24 Proliferative diabetic retinopathy in juvenile-onset type 1 diabetes, however, is not common during the first 10 years that a patient has diabetes.25 Management of ophthalmic manifestations of diabetes in children currently follows that of adults, with the use of intravitreal medications, laser photocoagulation, and surgery. Hypertensive retinopathy and anemic retinopathy are examples of other systemic diseases with retinal manifestations that generally improve with control of primary disease.26 Sickle cell retinopathy as well as hyperviscosity syndromes may manifest with retinal vascular occlusion, ischemia, and neovascularization, and may be locally treated with laser, cryotherapy, or surgical interventions if indicated.27,28
Metabolic diseases such as Niemann-Pick disease and Tay-Sachs disease result in abnormal buildup of metabolic products in the cellular retina that may manifest as a cherry red spot, which should prompt a detailed systemic examination and workup. Uyemura syndrome is described as a condition where white spots of the fundus occur in the setting of night blindness and xerosis secondary to vitamin A deficiency.29
Retinal findings may be the only manifestation of abusive head trauma (AHT), which has social, ethical, and medicolegal implications. It is often prudent to obtain fundus photographic documentation of multilayered retinal hemorrhages, and involvement of other medical and social services in such cases.
Fluorescein angiography may also prove beneficial in detecting areas of retinal ischemia and/or neovascularization. Terson syndrome is described as intraocular hemorrhage associated with traumatic brain injury or intracranial hemorrhage, and has been reported in individuals as early as 7 months of age.30 Purtscher retinopathy and Purtscher-like retinopathy are chorioretinopathy with a constellation of retinal findings such as retinal hemorrhages, cotton wool spots, optic disc edema, and inner retinal whitening. Purtscher retinopathy is typically associated with trauma,31 and Purtscher-like retinopathy has been described in pediatric patients with hemolytic uremic syndrome32 and juvenile dermatomyositis associated with thrombotic thrombocytopenic purpura.33
Respective characteristic retinal findings may prompt investigation for the presence of neurocutaneous syndromes, including neurofibromatosis, tuberous sclerosis (Bourneville syndrome), cerebrofacial angiomatosis (Sturge-Weber syndrome), retinal angiomatosis (von Hippel disease), ataxia-telangiectasia (Louis-Bar syndrome), and Wyburn-Mason syndrome. Retinal cavernous hemangioma is associated with CNS angiomas in von Hippel-Lindau syndrome.34
INFECTIOUS DISEASES
Toxoplasmosis, other, rubella, cytomegalovirus, and herpes (TORCH) infections are common causes of chorioretinitis and uveitis in children. Toxoplasmosis is the most common cause of pediatric posterior uveitis. Rubella, syphilis, cytomegalovirus (CMV), herpes virus, and HIV infections may all result in characteristic chorioretinal manifestations resulting in visual impairment. Lyme disease, tuberculosis, toxocariasis, histoplasmosis, candidiasis, cryptococcosis, cysticercosis, onchocerciasis, leptospirosis, and diffuse unilateral subacute neuroretinitis (DUSN) are known to cause pediatric retinal disease.
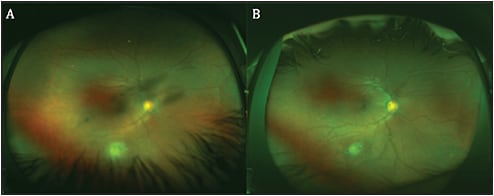
Treatment of infectious pediatric chorioretinitis and uveitis usually requires antimicrobial treatment. Peripheral toxoplasmosis retinochoroiditis may be observed clinically without intervention if stable, but may require treatment when associated with vitritis or decreased vision (Figure 1).
Antimicrobial treatments are usually administered by an intravitreal or systemic route, or a combination of both. Although discovery of new antimicrobial treatments has been limited, current antimicrobial treatments have remained largely effective. Limited case reports suggest that in CMV infection, infusion of CMV-specific leukocytes may be an effective treatment of both systemic disease and retinitis in patients resistant to standard therapies.35 In the immunosuppressed pediatric oncology population, this potentially provides an additional option in the treatment of CMV retinitis.
NONINFECTIOUS INFLAMMATORY CONDITIONS
Noninfectious inflammatory pediatric retinal disorders include sarcoidosis, Blau syndrome, Vogt-Koyanagi-Harada syndrome, Behcet’s disease, and sympathetic ophthalmia. These are treated mainly with a combination of local or systemic corticosteroids and steroid-sparing immunosuppressant therapies, such as methotrexate, mycophenolate mofetil, and newer biologic agents adalimumab and infliximab.36 Adalimumab received FDA approval for treatment of intermediate, posterior, and panuveitis in adults in June 2016. Good efficacy and acceptable side effect profiles have been reported in the treatment of uveitis in pediatric patients, especially in juvenile idiopathic arthritis uveitis cases refractory to other treatments.37-39
INTRAOCULAR TUMORS
Choroidal nevi and choroidal osteomas are examples of benign tumors that may be managed with close clinical observation. Other retinal lesions may be a clue to systemic associations and syndromes. For example, diffuse hemangioma of the choroid is associated with Sturge Weber syndrome, and congenital hyperplasia of the retinal pigment epithelium (CHRPE) in some cases may be associated with Gardner syndrome. Combined hamartoma of the retina and retinal pigment epithelium may be associated with neurofibromatosis type 2, incontinentia pigmenti, X-linked retinoschisis, and facial hemangiomas.
Retinoblastoma is a malignant tumor that arises from immature retinal cells. In the last century, retinoblastoma has gone from being a disease with >95% mortality to one in which a 99% survival rate is possible.40 This success in reducing mortality from retinoblastoma has largely been achieved with collective improvements in radiotherapy, intravitreal and systemic chemotherapy, and intra-arterial chemotherapy.41
CONCLUSION
We have discussed various available medical and surgical treatments for pediatric retinal disease. In the final section to follow, we will look at novel therapeutic strategies through the use of precision medicine, stem cell regenerative medicine, and other emerging therapies in the management of pediatric retinal disease. RP
REFERENCES
- Nicholson BP, Schachat AP. A review of clinical trials of anti-VEGF agents for diabetic retinopathy. Graefes Arch Clin Exp Ophthalmol. 2010;248(7):915-930.
- Rosenfeld PJ, Moshfeghi AA, Puliafito CA. Optical coherence tomography findings after an intravitreal injection of bevacizumab (Avastin) for neovascular age-related macular degeneration. Ophthalmic Surg Lasers Imaging. 2005;36(4):331-335.
- Sisk RA, Hufnagel RB, Bandi S, Polzin WJ, Ahmed ZM. Planned preterm delivery and treatment of retinal neovascularization in Norrie disease. Ophthalmology. 2014;121(6):1312-1313.
- Quiram PA, Drenser KA, Lai MM, Capone A Jr, Trese MT. Treatment of vascularly active familial exudative vitreoretinopathy with pegaptanib sodium (Macugen). Retina. 2008;28(3 Suppl):S8-S12.
- Tagami M, Kusuhara S, Honda S, Tsukahara Y, Negi A. Rapid regression of retinal hemorrhage and neovascularization in a case of familial exudative vitreoretinopathy treated with intravitreal bevacizumab. Graefes Arch Clin Exp Ophthalmol. 2008;246(12):1787-1789.
- Ramasubramanian A, Shields CL. Bevacizumab for Coats’ disease with exudative retinal detachment and risk of vitreoretinal traction. Br J Ophthalmol. 2012;96(3):356-359.
- Stergiou PK, Symeonidis C, Dimitrakos SA. Coats’ disease: treatment with intravitreal bevacizumab and laser photocoagulation. Acta Ophthalmol. 2009.87(6):687-688.
- Shah PK, Bachu S, Narendran V, Kalpana N, David J, Srinivas CR. Intravitreal bevacizumab for incontinentia pigmenti. J Pediatr Ophthalmol Strabismus. 2013;e52-e54.
- Thakar M, Bamrolia NR, Raina UK, Ghosh B. Intravitreal bevacizumab as an adjunct to vitrectomy in advanced Eales’ disease. J Ophthalmic Inflamm Infect. 2012;2(2):105-108.
- Moshiri A, Ha NK, Ko FS, Scott AW. Bevacizumab presurgical treatment for proliferative sickle-cell retinopathy-related retinal detachment. Retin Cases Brief Rep. 2013;7(3):204-205.
- Mintz-Hittner HA, Kennedy KA, Chuang AZ; BEAT-ROP Cooperative Group. Efficacy of intravitreal bevacizumab for stage 3+ retinopathy of prematurity. N Engl J Med. 2011;364(7):603-615.
- Quiroz-Mercado H, Martinez-Castellanos MA, Hernandez-Rojas ML, Salazar-Teran N, Chan RV. Antiangiogenic therapy with intravitreal bevacizumab for retinopathy of prematurity. Retina. 2008;28(3 Suppl):S19-S25.
- Jan SY, Choi KS, Lee SJ. Delayed-onset retinal detachment after an intravitreal injection of ranibizumab for zone 1 plus retinopathy of prematurity. J AAPOS. 2010;14(5):457-459.
- Kumar A, Sehra SV, Thirumalesh MB, Gogia V. Secondary rhegmatogenous retinal detachment following intravitreal bevacizumab in patients with vitreous hemorrhage or tractional retinal detachment secondary to Eales’ disease. Graefes Arch Clin Exp Ophthalmol. 2012;250(5):685-690.
- Patwardhan SD, Azad R, Shah BM, Sharma Y. Role of intravitreal bevacizumab in Eales disease with dense vitreous hemorrhage: a prospective randomized control study. Retina. 2011;31(5):866-870.
- Honda S, Hirabayashi H, Tsukahara Y, Negi A. Acute contraction of the proliferative membrane after an intravitreal injection of bevacizumab for advanced retinopathy of prematurity. Graefes Arch Clin Exp Ophthalmol. 2008;246(7):1061-1063.
- Moshfeghi DM, Berrocal AM. Retinopathy of prematurity in the time of bevacizumab: incorporating the BEAT-ROP results into clinical practice. Ophthalmology. 2011;118(7):1227-1228.
- Sato T, Wada K, Arahori H, et al. Serum concentrations of bevacizumab (avastin) and vascular endothelial growth factor in infants with retinopathy of prematurity. Am J Ophthalmol. 2012;153(2):327-333.
- Trese MT, Drenser KA, Capone A. Angiogenesis and angiomaintenance in pediatric retinal diseases. Ret Physician. 2011;8(3). Available at http://www.retinalphysician.com/issues/2011/april-2011/angiogenesis-and-angiomaintenance-in-pediatric-ret
- Komiya Y, Habas R. Wnt signal transduction pathways. Organogenesis. 2008;4(2):68-75.
- Sızmaz S, Yonekawa Y, Trese MT. Familial exudative vitreoretinopathy. Turk J Ophthalmol. 2015;45(4):164-168.
- Nikopoulos K, Venselaar H, Collin RW, et al. Overview of the mutation spectrum in familial exudative vitreoretinopathy and Norrie disease with identification of 21 novel variants in FZD4, LRP5, and NDP. Hum Mutat. 2010;31(6):656-666.
- Pelcastre EL1, Villanueva-Mendoza C, Zenteno JC. Novel and recurrent NDP gene mutations in familial cases of Norrie disease and X-linked exudative vitreoretinopathy. Clin Exp Ophthalmol. 2010;38(4):367-374.
- Forlenza GP, Stewart MW. Diabetic retinopathy in children. Pediatr Endocrinol Rev. 2012;10(2):217-226.
- Krolewski AS, Warram JH, Rand LI, Christlieb AR, Busick EJ, Kahn CR. Risk of proliferative diabetic retinopathy in juvenile-onset type I diabetes: a 40-yr follow-up study. Diabetes Care. 1986;9(5):443-452.
- Foster BJ, Ali H, Mamber S, Polomeno RC, Mackie AS. Prevalence and severity of hypertensive retinopathy in children. Clin Pediatr (Phila). 2009;48(9):926-930.
- Condon PI, Serjeant GR. Ocular findings in homozygous sickle cell anemia in Jamaica. Am J Ophthalmol. 1972;73(4):533-543.
- Rosenberg JB, Hutcheson KA. Pediatric sickle cell retinopathy: correlation with clinical factors. J AAPOS. 2011;15(1):49-53.
- Fuchs A. White spots of the fundus combined with night blindness and xerosis (Uyemura’s syndrome). Am J Ophthalmol. 1959;48(1, Part 1):101-103.
- Bhardwaj G, Jacobs MB, Moran KT, Tan K. Terson syndrome with ipsilateral severe hemorrhagic retinopathy in a 7-month-old child. J AAPOS. 2010;14(5):441-443.
- Tomasi LG, Rosman NP. Purtscher retinopathy in the battered child syndrome. Am J Dis Child. 1975;129(11):1335-7.
- Lauer AK, Klein ML, Kovarik WD, Palmer EA. Hemolytic uremic syndrome associated with Purtscher-like retinopathy. Arch Ophthalmol. 1998;116(8):1119-1120.
- Bader-Meunier B, Monnet D, Barnerias C, et al. Thrombotic microangiopathy and Purtscher-like retinopathy as a rare presentation of juvenile dermatomyositis. Pediatrics. 2012;129(3):e821-e824.
- Magee MA1, Kroll AJ, Lou PL, Ryan EA. Retinal capillary hemangiomas and von Hippel-Lindau disease. Semin Ophthalmol. 2006;21(3):143-150.
- Gupta MP, Coombs P, Prockop SE, et al. Treatment of cytomegalovirus retinitis with cytomegalovirus-specific T-lymphocyte infusion. Ophthalmic Surg Lasers Imaging Retina. 2015;46(1):80-82.
- Pasadhika S, Rosenbaum JT. Update on the use of systemic biologic agents in the treatment of noninfectious uveitis. Biologics. 2014;8:67-81.
- Biester S1, Deuter C, Michels H, et al. Adalimumab in the therapy of uveitis in childhood. Br J Ophthalmol. 2007;91(3):319-324.
- Castiblanco C, Meese H, Foster CS. Treatment of pediatric uveitis with adalimumab: the MERSI experience. J AAPOS. 2016;20(2):145-147.
- Simonini G, Taddio A, Cattalini M, et al. Superior efficacy of Adalimumab in treating childhood refractory chronic uveitis when used as first biologic modifier drug: Adalimumab as starting anti-TNF-alpha therapy in childhood chronic uveitis. Pediatr Rheumatol Online J. 2013;11:16.
- Abramson DH. Retinoblastoma: saving life with vision. Annu Rev Med. 2014;65:171-184.
- Gobin YP, Dunkel IJ, Marr BP, Brodie SE, Abramson DH. Intra-arterial chemotherapy for the management of retinoblastoma: four-year experience. Arch Ophthalmol. 2011;129(6):732-737.