







Pediatric retinal conditions require special consideration because of the unique pathologic spectrum of this patient population. Ophthalmoscopic retinal examination as well as diagnostic and therapeutic procedures in pediatric patients can be challenging due to reduced patient cooperation, and surgical techniques may differ in pediatric eyes due to anatomical differences from adult eyes.1
Pediatric retinal conditions are categorized into developmental abnormalities, congenital or acquired vascular diseases, infections, noninfectious inflammatory disorders, tumors, and systemic diseases with retinal manifestations (Table 1). Although retinopathy of prematurity is a leading cause of childhood blindness, the focus of this 3-part series will be on non-ROP pediatric retinal conditions. We will explore current diagnostic and management strategies and will discuss potential future therapies for pediatric retinal disease.
| CATEGORY | DISEASE |
|---|---|
| Vasoproliferative or vascular | Coats disease, Eales disease, incontinentia pigmenti, retinopathy of prematurity, Norrie disease, familial exudative vitreoretinopathy |
| Infections | Toxoplasmosis, cytomegalovirus, herpes simplex virus, varicella zoster virus, human immunodeficiency virus, rubella, syphilis, Lyme disease, tuberculosis, toxocariasis |
| Noninfectious inflammatory disorders | Sarcoidosis, Blau syndrome (familial juvenile systemic granulomatosis), Vogt-Koyanagi-Harada syndrome, Behçet disease, scleritis, granulomatosis with polyangiitis, sympathetic ophthalmia |
| Tumors and neoplasia | Choroidal nevi, choroidal osteoma, diffuse hemangioma (Sturge Weber), congenital hyperplasia of retinal pigment epithelium, combined hamartoma of the retina and RPE, retinoblastoma, leukemia/lymphoma, malignant melanoma |
| Syndromes and systemic diseases with retinal manifestations | Diabetes, hypertension, anemia, hyperviscosity syndrome, sickle cell disease, Stickler syndrome, Terson syndrome, Purtscher and Purtscher-like retinopathy, neurofibromatosis, tuberous sclerosis, cerebrofacial angiomatosis, retinal angiomatosis, ataxia-telangiectasia, Wyburn-Mason syndrome |
| Other | Persistent fetal vasculature, abusive head trauma, cone dystrophies, cone-rod dystrophies, X-linked retinoschisis |
DIAGNOSTIC AND IMAGING MODALITIES IN PEDIATRIC RETINAL CONDITIONS
Advancing technologies in diagnostic and imaging modalities increasingly influence treatment of pediatric retinal conditions. Traditionally, pediatric retinal disease was primarily diagnosed with clinical examination by indirect ophthalmoscopy and documented over time with retinal drawings. Fundus imaging systems have improved tremendously in recent years, enabling high-resolution photographic documentation of the retina. Older imaging systems, such as the NM-200D camera (NIDEK, Inc.) had approximately a 30° field of view. Now contact imaging systems, like the RetCam (Clarity Medical Systems), Panocam (Visunex Medical Systems), and 3nethra neo (Forus Health) that provide a wider field of view are very useful for documentation of fundus findings in the clinic, at the bedside, and during examinations under anesthesia.
Ultrawidefield imaging with the Optos imaging systems (Optos PLC), can provide up to a 200° field of view. These systems are noncontact and allow for quality images to be obtained, particularly in the outpatient clinical setting. Ultrawidefield imaging has been used successfully in combination with ultrawidefield fluorescein angiography in pediatric retinal disease, very often avoiding the need for examination under anesthesia and assisting in the documentation, evaluation, and treatment of pediatric retinal pathology.2,3
Optical coherence tomography has revolutionized imaging of the retinal architecture. Time-domain OCT systems have been superseded by newer spectral-domain OCT systems with ultrahigh resolution of up to 2-3 micrometers.4 Envisu (Leica) is a handheld, noncontact SD-OCT system that has been shown to aid in retinal evaluation during examinations under anesthesia,5,6 thus extending OCT technology to include the pediatric population. In the future, OCT angiography may prove useful in the diagnosis and management of pediatric retinal conditions.
SURGERY, LASER, AND CRYOTHERAPY IN PEDIATRIC RETINAL DISEASE
Anatomical Considerations for Surgery
When managing pediatric retina patients, certain anatomical differences between adults and children need to be considered. In very young children, the eye is grossly smaller than the adult eye. The ratio of the size of the lens to the eye is larger, and pediatric vitreoretinal surgeons have to be very mindful of the lens during intravitreal injections, trocar insertion, and instrument manipulation in order to minimize the risk of traumatic lens injury. The pediatric sclera has a different elasticity compared to adults, and sclerotomy sites may not always be amenable to being sutureless after vitrectomy. The attachment of the pediatric cortical vitreous to the internal limiting lamina of the retina is known to be much stronger in younger patients.1 This contributes to challenges in removing the vitreous, and increased difficulty with inducing a posterior vitreous detachment. A recent randomized, placebo-controlled study of intravitreal ocriplasmin administered 30 minutes to 60 minutes prior to vitrectomy in pediatric patients did not exhibit clear efficacy with inducing posterior vitreous detachment before vitrectomy or after application of suction, but this study was limited by a small sample size.7 Postoperatively, younger patients can have a more robust inflammatory response, potentially resulting in higher rates of proliferative vitreoretinopathy and associated complications.8-10 Also, the possibility that children will not comply with appropriate postoperative head positioning may favor the use of silicone oil over intraocular gases as intraocular tamponades.11
Laser and Cryotherapy
Laser photocoagulation and cryotherapy are used in the treatment of a wide range of pediatric retinal conditions. In retinal neovascular diseases, laser or cryotherapy destroys avascular or ischemic retina, decreasing the ischemic and neovascular drive.12,13 In retinal tears or detachments, both laser photocoagulation and cryotherapy result in chorioretinal scarring and adhesion sealing the retinal break(s). Selection of laser wavelength and parameters depend on the indication for treatment, fundus pigmentation, and clarity of the ocular media.
Clinical Examples
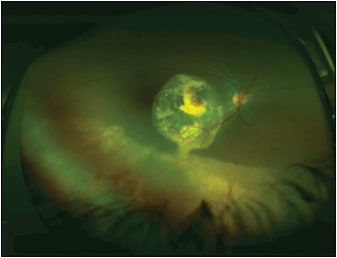
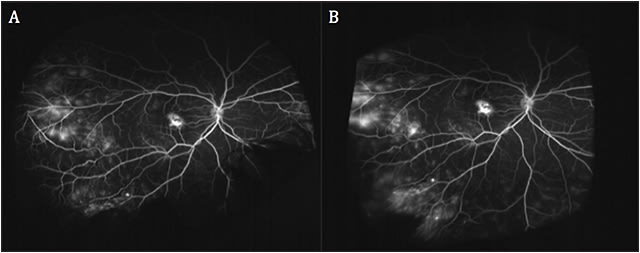
Widefield color fundus and fundus fluorescein angiogram images in Figures 1 and 2 illustrate the abnormal retinal vasculature, telangiectasias, hemorrhages, and exudative deposits characteristic in Coats disease. Laser photocoagulation with a wavelength of 532 nm was chosen for the treatment of this case of Coats disease.
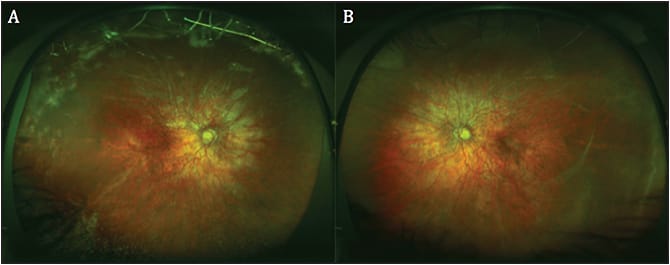
Stickler syndrome is a connective tissue disorder associated with abnormal production of types II, IX and XI collagen.14 These patients have an increased rate of retinal tears and detachments that often manifest during childhood.15 Figure 3 includes fundus images of a patient with Stickler syndrome who required pars plana vitrectomy, endolaser, and silicone oil tamponade for rhegmatogenous retinal detachment associated with a giant retinal tear.
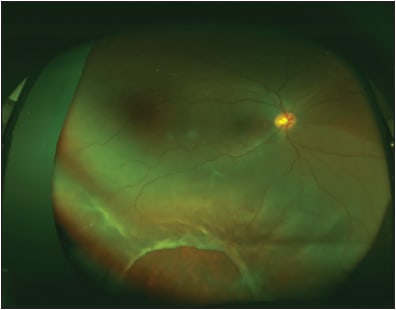
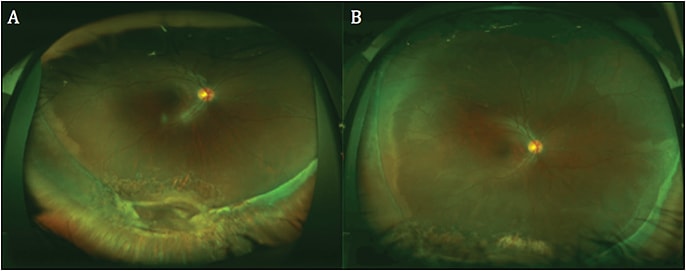
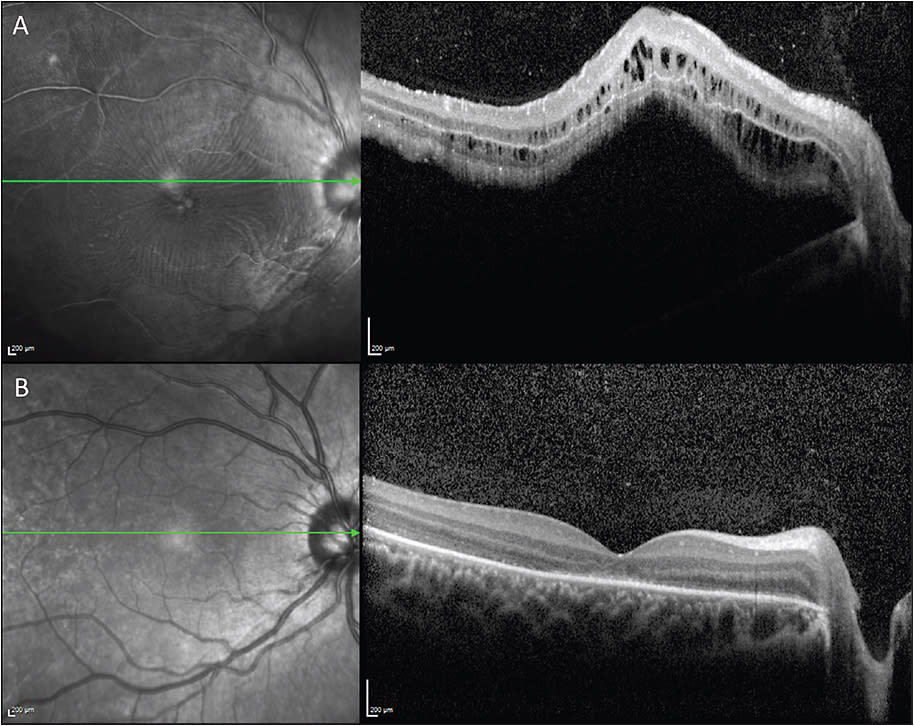
Scleral buckles, in conjunction with the creation of chorioretinal adhesions around retinal breaks with laser photocoagulation or cryotherapy, may be a favorable primary treatment option for rhegmatogenous retinal detachments in younger individuals. The fundus (Figures 4 and 5) and OCT (Figure 6) images illustrate a large inferior retinal tear and rhegmatogenous retinal detachment that resolved after treatment with a scleral buckle and cryotherapy. Successful treatment of rhegmatogenous retinal detachments with primary scleral buckling may reduce the risk of secondary cataract formation associated with vitrectomy.
Conclusion
Diagnostic and imaging technology continue to improve and impact clinical management of pediatric retinal diseases. Understanding the anatomic differences between pediatric and adult eyes is crucial for effective surgical and medical treatment of pediatric vitreoretinal pathology. In the next chapter of this series, we will discuss the therapeutic modalities available for the management of pediatric retinal disease.
REFERENCES
- Sebag J. Age-related differences in the human vitreoretinal interface. Arch Ophthalmol. 1991;109(7):966-971.
- Kang KB, Wessel MM, Tong J, D’Amico DJ, Chan RV. Ultra-widefield imaging for the management of pediatric retinal diseases. J Pediatr Ophthalmol Strabismus. 2013;50(5):282-288.
- Tsui I, Franco-Cardenas V, Hubschman JP, Schwartz SD. Pediatric retinal conditions imaged by ultra wide field fluorescein angiography. Ophthalmic Surg Lasers Imaging Retina. 2013;44(1):59-67.
- Drexler W, Morgner U, Ghanta RK, Kärtner FX, Schuman JS, Fujimoto JG. Ultrahigh-resolution ophthalmic optical coherence tomography. Nat Med. 2001;7(4):502-507.
- Scott AW, Farsiu S, Enyedi LB, Wallace DK, Toth CA. Imaging the infant retina with a hand-held spectral-domain optical coherence tomography device. Am J Ophthalmol. 2009;147(2):364-373.
- Vinekar A, Mangalesh S, Jayadev C, Maldonado RS, Bauer N, Toth CA. Retinal imaging of infants on spectral domain optical coherence tomography. Biomed Res Int. 2015;782420.
- Drenser K, Girach A, Capone A Jr. A randomized, placebo-controlled study of intravitreal ocriplasmin in pediatric patients scheduled for vitrectomy. Retina. 2016;36(3):565-575.
- Akabane N, Yamamoto S, Tsukahara I, et al. Surgical outcomes in juvenile retinal detachment. Jpn J Ophthalmol. 2001;45(4):409-411.
- Fivgas GD, Capone A Jr. Pediatric rhegmatogenous retinal detachment. Retina. 2001;21(2):101-106.
- Yokoyama T, Kato T, Minamoto A, et al. Characteristics and surgical outcomes of paediatric retinal detachment. Eye (Lond). 2004;18(9):889-892.
- Scott IU, Flynn HW Jr, Azen SP, Lai MY, Schwartz S, Trese MT. Silicone oil in the repair of pediatric complex retinal detachments: a prospective, observational, multicenter study. Ophthalmology. 1999;106(7):1399-1407.
- Hunter DG, Repka MX. Diode laser photocoagulation for threshold retinopathy of prematurity. A randomized study. Ophthalmology. 1993;100(2):238-244.
- Schefler AC, Berrocal AM, Murray TG. Advanced Coats’ disease. Management with repetitive aggressive laser ablation therapy. Retina. 2008;28(3 Suppl):S38-S41.
- Ang A, Poulson AV, Goodburn SF, Richards AJ, Scott JD, Snead MP. Retinal detachment and prophylaxis in type 1 Stickler syndrome. Ophthalmology. 2008;115(1):164-168.
- Snead MP, Yates JR. Clinical and Molecular genetics of Stickler syndrome. J Med Genet. 1999;36(5):353-359.