







Current Concepts in Diagnosis and Management of Central Retinal Artery Occlusion
Timely diagnosis is essential to preserve vision.
MARGARET A. GREVEN, MD • STEPHEN J. SMITH, MD
Central retinal artery occlusion (CRAO), first described by Von Graefe in 1859, is characterized by sudden, painless loss of vision due obstruction of the central retinal artery, which supplies blood to the inner retina.1
Analogous to a cerebral stroke, CRAO is most often caused by emboli originating from carotid atherosclerosis, but it may also occur secondary to cardiac or other emboli, vasculitis, thrombosis, or trauma.2 The prevalence of CRAO is approximately 1:100,000,3 and risk factors include hypertension, diabetes mellitus, cardiac disease, hypercoagulability, and tobacco use.
Obstruction of the central retinal artery results in inner retinal ischemia with relative outer retinal sparing due to dual retinal circulation, with the central retinal artery, a branch of the ophthalmic artery, supplying the inner retinal layers and the choriocapillaris of the choroid supplying the outer retinal layers.
A variation of this condition occurs in approximately 30% of individuals who have a cilioretinal artery, a branch of the posterior ciliary artery, which supplies a part of the macula in the papillomacular bundle.4 Depending on the extent of the macula supplied by the cilioretinal artery, visual acuity may not be affected as severely or at all in CRAO.
Margaret A. Greven, MD, and Stephen J. Smith, MD, serve on the faculty of the Stanford University School of Medicine in Palo Alto, CA. Neither author reports any financial interests in products mentioned in this article. Dr. Greven can be reached via e-mail at margaret.greven@gmail.com.
CRAO, although relatively uncommon, is an important cause of visual morbidity and functional loss. Timely diagnosis allows for the recognition and modification of underlying atherosclerotic and vascular risk factors that could lead to cerebral stroke, and it also enables expedited intervention to be undertaken, although no consensus currently exists regarding CRAO treatment efficacy. This article reviews the diagnosis, natural history, and treatment of CRAO.
DIAGNOSIS
Initial diagnosis is based primarily on history and clinical examination findings. Patients present with acutely decreased vision in one eye, afferent pupillary defect, retinal pallor, cherry-red spot, and vascular attenuation or boxcarring of the retinal blood vessels. Vision is most often Snellen 20/400 or worse in the affected eye. A refractile embolus, or Hollenhorst plaque, may also be visible within the central retinal artery at the disc or in more distal arterial branches.
Imaging
Imaging can aid in the diagnosis of CRAO. Fluorescein angiography in acute CRAO typically demonstrates delayed retinal artery filling, arteriolar attenuation, and rarely complete absence of retinal artery perfusion. In some cases, FA may appear normal if perfusion has been restored.
Figure 1 shows fundus photography and FA in a patient with acute CRAO. FA is useful to differentiate arteritic from nonarteritic CRAO because the choroidal circulation is often affected in arteritic CRAO, but it is very rarely involved in nonarteritic CRAO.
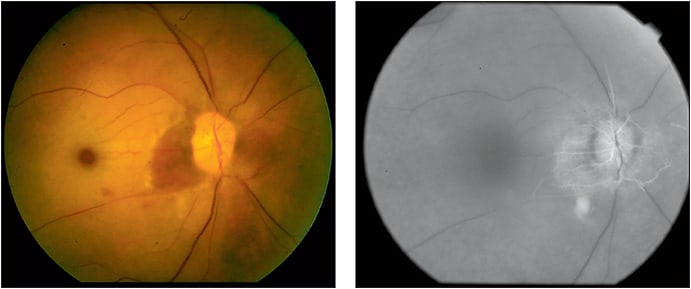
Figure 1. Fundus photograph (left) of right eye with central retinal artery occlusion notable for retinal pallor, cherry red spot in the central macula, and small area of perfused retina in the nasal macula consistent with cilioretinal artery sparing. Fluorescein angiography (right) shows slow filling of the retinal arteries with perfusion of the small macular area supplied by the cilioretinal artery.
Optical coherence tomography in acute CRAO is notable for inner retinal hyper-reflectivity and thickening, with corresponding shadowing of the outer retinal layers. Figure 2 shows fundus photography and corresponding OCT in acute CRAO. In chronic CRAO, OCT shows inner retinal atrophy.
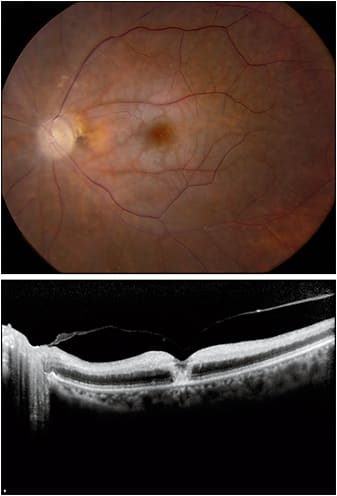
Figure 2. Fundus photo (top) of a left eye with central RAO showing macular pallor and cherry red spot, as well as attenuated arteries. OCT (bottom) of the same patient demonstrates inner retinal hyperreflectivity and thickening.
Electroretinography (ERG) in CRAO characteristically shows reduction of the b-wave due to inner retinal damage, with relative preservation of the a-wave, resulting in an electronegative ERG.5
Postdiagnostic Testing
Once the diagnosis of CRAO is made, testing is undertaken to identify treatable risk factors and to identify any potential embolic source. Vascular risk factors can be evaluated with a careful history and physical examination, blood pressure, fasting glucose, and fasting lipids. Carotid ultrasound or magnetic resonance angiography of the neck and transthoracic or transesophageal echocardiography are useful to evaluate for embolic sources.
If clinical suspicion warrants, workup for giant cell arteritis is performed, including erythrocyte sedimentation rate, C-reactive protein, and platelet count. In young patients or patients without vascular risk factors, consideration should be given to undertaking a hypercoagulable and vasculitic workup.6,7 The suggested workup for CRAO is outlined in the Table.
| SUGGESTED TESTING | |
|---|---|
| All patients | Blood pressure
Fasting lipid panel Fasting blood glucose |
| Suspicion for giant cell arteritis | Erythrocyte sedimentation rate
C-reactive protein Platelets Temporal artery biopsy |
| Embolic | Carotid ultrasonography or magnetic resonance angiography of the neck
Transthoracic or transesophageal echocardiography |
| Patients <50 years of age or without vascular risk factors | Hypercoagulability:
factor V Leiden, protein C, protein S, antithrombin III, antiphosopholipid, anticardiolipin, homocysteine, serum protein electrophoresis, fibrinogen, lipoprotein(a), factor VIIIC, plasminogen activity, factor II gene polymorphism Inflammatory: ANA, ANCA, RPR, FTA-Abs |
PROGNOSIS AND NATURAL HISTORY
CRAO can be divided into four different subtypes: permanent nonarteritic; transient nonarteritic; nonarteritic with cilioretinal sparing; and arteritic. These subtypes are associated with different presenting VAs and different spontaneous recovery rates. The subtype with the worst presenting vision is arteritic CRAO, followed by permanent CRAO, then transient CRAO, and finally CRAO with cilioretinal sparing.8
In one study of 260 patients with CRAO, patients with transient CRAO and cilioretinal artery-sparing CRAO had the best prognosis for visual improvement, with 82% and 67% of patients, respectively, showing VA improvement over the first week after onset.8 In contrast, only 22% of patients with permanent CRAO manifested VA improvement at one week, and no patients with arteritic CRAO improved.8
In all subtypes of CRAO except for arteritic, spontaneous recovery can be observed as part of the natural history of the condition, which is an important consideration when evaluating the success of treatments for CRAO.
Hayreh and Zimmerman9 performed experiments examining inner retinal perfusion in a model of CRAO in young healthy rhesus monkeys. They showed that retinal survival time after clamping of the central retinal artery was approximately 97-98 minutes. Retinal damage sustained with shorter nonperfusion times was reversible.9 After 105 minutes, irreversible retinal damage occurred in healthy monkeys.9
In a follow-up study carried out in old, atherosclerotic rhesus monkeys, no retinal damage was detected before 97 minutes of occlusion, but after that time, the longer the CRAO was, the more retinal damage was sustained.10 In this study, 240 minutes after induced CRAO, massive irreversible retinal damage occurred.10 The paradoxical finding of a longer window before permanent ischemic damage in the older monkeys may be explained by compensatory mechanisms already in effect in the atherosclerotic monkeys, which were protective and allowed for longer retinal survival times.
Although these findings in rhesus monkeys cannot be directly extrapolated to give exact retinal survival times in humans, they suggest that there is a period of time after a CRAO occurs that retinal damage is reversible, and after a certain amount of time elapses, irreversible damage occurs.
Taking this process into account, to be effective at restoring vision, any treatment for CRAO must be performed prior to the occurrence of irreversible retinal damage, which likely occurs within a few hours of symptom onset.
TREATMENT
Conventional
Conventional therapies for CRAO have focused on decreasing intraocular pressure and/or vasodilation to dislodge the causative embolus and move it downstream to reperfuse the retina.
Suggested therapies include anterior-chamber paracentesis, ocular antihypertensives, and intravenous or oral acetazolamide to lower IOP and increase retinal artery perfusion; ocular massage to dislodge emboli manually; sublingual isosorbide dinitrate, oral pentoxifylline, inhalation of carbogen, and hyperbaric oxygen to increase blood oxygen content and dilate retinal arteries; or a combination of the aforementioned treatments.11-22
Although case reports, retrospective studies, and nonrandomized, noncontrolled studies have reported success with these modalities in individual patients, most have not been evaluated with randomized, controlled trials.
Only two randomized, controlled trials have been published to date to evaluate the effectiveness of conventional CRAO treatments. The first compared hemodilution alone to hemodilution combined with enhanced external counterpulsation (EEC), a technique involving intermittent leg compression in synch with the cardiac cycle, which is believed to improve cardiac output and end-organ perfusion. The study included 20 patients with either CRAO or branch RAO, with a duration of less than five days.
At 48 hours after the intervention, there was improved perfusion of ischemic retina in the patients who received EEC compared to controls, but this difference was not sustained. Furthermore, no corresponding improvement in VA was observed in association with the improved perfusion.23
The second randomized, controlled trial included 10 patients with sudden vision loss from CRAO and compared placebo to oral pentoxyfylline, a phosphodiesterase inhibitor thought to increase red blood cell deformability and lead to vasodilation. The authors did not specify the duration of vision loss in these patients.
After four weeks of treatment, both groups had improvement in blood flow velocity, but those receiving pentoxyfylline had significantly more improvement than control patients. However, pentoxifylline-treated patients did not experience corresponding improvement in VA despite improved perfusion.24
These two trials were both small, and neither demonstrated efficacy in terms of visual improvement of the treated patients. Importantly, both trials included patients who likely were outside the window for clinical efficacy, making visual improvement unlikely even with an effective intervention. To date, conventional treatments have not been proved to have benefit, compared to observation for CRAO.
Thrombolysis
Thrombolysis, a well-established treatment for stroke and acute myocardial infarction, has also been investigated for the treatment of CRAO. With the goal of clot lysis and restoration of perfusion, a thrombolytic agent can either be administered intravenously or be delivered directly into the ophthalmic artery in local intra-arterial fibrinolysis (LIF).
LIF was first reported for treatment of CRAO in 1984, and since then, its use has been supported by several retrospective studies.25-28 One retrospective case-control study found that patients treated with LIF earlier than four hours after onset of symptoms had significantly better visual improvement than those treated later.27 This result was consistent with Hayreh’s rhesus monkey studies, which showed a short duration of retinal survival following CRAO.9,10
Another retrospective, case-control study of 42 patients with CRAO of less than 15 hours of duration showed a statistically significant visual improvement in patients who received LIF in small aliquots until patency of the central retinal artery was established compared to controls, and the only complication was groin hemorrhage in two of the patients receiving LIF.28
The EAGLE study was a multicenter, randomized, controlled trial that compared LIF to conservative treatment (ocular massage, topical beta blocker, acetazolamide, aspirin, heparin, and/or hemodilution).29 The 84 patients included in the study had CRAO of <20 hours’ duration and poor VA.
The primary endpoint was VA at one month, and although both groups experienced clinically significant VA improvement, there was no difference between the groups. There was, however, a significantly higher rate of adverse events in the LIF group, including cerebral hemorrhage (37% compared to 4.3% in controls).29 Due to the high rate of adverse events, the study was discontinued early, and the authors recommended against LIF in CRAO.30
Critics of the EAGLE study have emphasized the 20-hour duration of symptoms as likely outside the therapeutic window for treatment of CRAO.31 Lack of baseline neuroimaging in the EAGLE study makes excluding pre-existing cerebral infarcts impossible, and hemorrhagic transformation of pre-existing infarcts could have accounted for high rates of cerebral hemorrhage in the LIF-treated patients.32
Finally, thrombolytic agents are likely only effective at dissolving fibrin-platelet clots, which are believed to account for only 15% of clots in CRAO, with 74% composed of cholesterol and 10% composed of calcified material.31,33
Intravenous thrombolysis has also been investigated for the treatment of CRAO. In one prospective study, 28 patients were treated with intravenous tissue plasminogen activator (t-PA) and intravenous heparin to prevent reocclusion of the central retinal artery. At baseline, patients had VA of 20/100 or worse and symptom onset of less than 12 hours prior to treatment.
Of the 17 eyes treated prior to 6.5 hours of symptom onset, seven (40%) had final vision of 20/50 or better, compared to none of the patients with symptoms for longer than 6.5 hours prior to treatment, and no patients had adverse effects.34 The finding of better outcomes in patients treated earlier lends additional support to Hayreh’s theory of retinal survival time.
In a small, randomized, controlled trial, intravenous t-PA was compared to intravenous saline in patients with CRAO presenting within 24 hours of symptom onset. There were eight patients in each arm of the study.
Two patients (25%) in the treatment group had visual improvement of 3 lines or more at one week. Both of these patients had a duration of symptoms of less than six hours. Unfortunately, visual improvement was not sustained long term due to reocclusion of the central retinal artery. One patient sustained intracranial hemorrhage. The authors concluded that reocclusion might require adjuvant anticoagulation and that the window for intervention in CRAO is likely to be less than six hours.35
Schrag et al performed a meta-analysis to compare intravenous thrombolytic therapy, conservative therapy (ocular massage, anterior-chamber paracentesis, and/or hemodilution), and no treatment (natural history). Intravenous thrombolysis showed a benefit compared to the natural history group if delivered before 4.5 hours of symptom onset, while patients undergoing conservative treatment had worse VA outcomes than the natural history group.36
Of the 147 patients treated with fibrinolytic therapy, there were five patients with major hemorrhages, and four of them were treatment-related fatalities from a single trial using an unclear dose of IV streptokinase. The authors concluded that a trial of early systemic fibrinolytic therapy is warranted and that conservative treatments may in fact be harmful.36
In theory, the ideal candidate for treatment with t-PA is a patient with a fibrin-platelet clot, CRAO with duration of less than four hours, and normal neuroimaging. However, a randomized, controlled trial of fibrinolysis in such a group of patients has yet to be performed. In light of the current data, any decision to perform fibrinolysis for CRAO must be made after a detailed discussion of the potentially life-threatening risks of fibrinolysis.
Arteritic CRAO
For cases of CRAO attributable to giant cell arteritis, intravenous steroids should be initiated as soon as possible. Unfortunately, the prognosis for recovery of vision in patients with arteritic CRAO is essentially nonexistent, but with timely recognition and institution of steroid treatment, vision loss can be prevented in the fellow eye.37
Long-term Management
As with other vascular-occlusive conditions, one potential complication of CRAO is retinal or anterior-segment neovascularization, which can lead to complications such as neovascular glaucoma and vitreous hemorrhage.
Neovascularization can occur in up to 14% to 18% of patients who have had CRAO,38,39 and it was reported to occur within two to 16 weeks of symptom onset, with an average of 8.5 weeks.39
For this reason, close monitoring following the acute event is recommended. If neovascularization is noted, treatment with panretinal photocoagulation is undertaken to induce regression of neovascularization and prevent its complications.
CONCLUSION
CRAO is a relatively rare condition that often leads to catastrophic loss of vision. Although numerous treatment strategies have been proposed, there is a lack of convincing evidence as to their benefit. In addition, more invasive therapies, such as thrombolysis, carry the potential for serious adverse events, including fatal intracranial hemorrhage.
For these reasons, most clinicians currently employ conservative treatment or observation to manage patients with CRAO. Even if a safe and reliable treatment is confirmed for CRAO, its application will be limited due to the short therapeutic window for retinal recovery following CRAO. Management of CRAO risk factors, including hypertension, cholesterol, cardiovascular disease, and diabetes mellitus, is important to reduce the incidence of CRAO. RP
REFERENCES
1. Von Graefe A. Central retinal artery embolism as a cause of sudden blindness. Arch Ophthalmol. 1859;5:136-157.
2. Hayreh SS, Podhajsky PA, Zimmerman MB. Retinal artery occlusion: associated systemic and ophthalmic abnormalities. Ophthalmology. 2009;116:1928-1936.
3. Brown GC. Retinal arterial obstructive disease. In: Ryan SJ, ed. Retina, vol 2. St Louis, MO; CV Mosby Co; 1989:403-419.
4. Justice J Jr, Lehmann RP. Cilioretinal arteries. Cilioretinal arteries. A study based on review of stereo fundus photographs and fluorescein angiographic findings. Arch Ophthalmol. 1976;94:1355-1358.
5. Lima LH, Cella W, Brue C, Tsang SH. Unilateral electronegative ERG in a presumed central retinal artery occlusion. Clin Ophthalmol. 2010;4:1311-1314.
6. Nagy V, Takacs L, Steiber Z, et al. Thrombophilic screening in retinal artery occlusion patients. Clin Ophthalmol. 2008;2:557-561.
7. Ratra D, Dhupper M. Retinal arterial occlusions in the young: systemic associations in Indian population. Indian J Ophthalmol. 2012;60:95-100.
8. Hayreh SS, Zimmerman MB. Central retinal artery occlusion: visual outcome. Am J Ophthalmol. 2005;140:376-391.
9. Hayreh SS, Kolder HE, Weingeist TA. Central retinal artery occlusion and retinal tolerance time. Ophthalmology. 1980;87:75-78.
10. Hayreh SS, Zimmerman B, Kimura A, Sanon A. Central retinal artery occlusion. Retinal survival time. Exp Eye Res. 2004;78:723-736.
11. Rumelt S, Brown GC. Update on treatment of retinal arterial occlusions. Curr Opin Ophthalmol. 2003;14:139-141.
12. Rassam S, Patel V, Kohner E. The effect of acetazolamide on retinal circulation. Eye (Lond). 1993;7:697-702.
13. Rumelt S, Dorenboim Y, Rehany U. Aggressive systematic treatment for central retinal artery occlusion. Am J Ophthalmol. 1999;128:733-738.
14. Harino S, Grunwald JE, Petrig BJ, Riva CE. Rebreathing into a bag increases human retinal macular blood velocity. Br J Ophthalmol. 1995;79:380-383.
15. Deutsch TA, Read JS, Ernest JT, Goldstick TK. Effects of oxygen and carbon dioxide on the retinal vasculature in humans. Arch Ophthalmol. 1983;101:1278-1280.
16. Beiran I, Goldenberg I, Adir Y, Tamir A, Shupak A, Miller B. Early hyperbaric oxygen therapy for retinal artery occlusion. Eur J Ophthalmol. 2001;11:345-350.
17. Weinberger AW, Siekmann UP, Wolf S, Rossaint R, Kirchhof B, Schrage NF. Treatment of acute central retinal artery occlusion (CRAO) by hyperbaric oxygenation therapy (HBO) - Pilot study with 21 patients. Klin Monbl Augenheilkd. 2002;219:728-734.
18. Aisenbrey S, Krott R, Heller R, Krauss D, Rössler G, Heimann K. Hyperbaric oxygen therapy in retinal artery occlusion. Ophthalmologe. 2000;97:461-467.
19. Canan H, Ulas B, Altan-Yaycioglu R. Hyperbaric oxygen therapy in combination with systemic treatment of sickle cell disease presenting as central retinal artery occlusion: a case report. J Med Case Rep. 2014;8:370.
20. Nanjiani MA. Total central retinal artery occlusion successfully treated. Br Med J. 1966;1:32.
21. Varma DD, Cugati S, Lee AW, et al. A review of central retinal artery occlusion: clinical presentation and management. Eye (Lond). 2013;27:688-697.
22. Gilbert AL, Choi CC, Lessell S. Acute management of central retinal artery occlusion. Int Ophthalmol Clin. 2015;55:157-166.
23. Werner D, Michalk F, Harazny J, et al. Accelerated reperfusion of poorly perfused retinal areas in central retinal artery occlusion and branch retinal artery occlusion after a short treatment with enhanced external counterpulsation. Retina. 2004;24:541-547.
24. Incandela L, Cesarone MR, Belcaro G, et al. Treatment of vascular retinal disease with pentoxifylline: a controlled, randomized trial. Angiology. 2002;53(Suppl 1):S31-S34.
25. Theron J, Courtheoux P, Casasco A, et al. Local intraarterial fibrinolysis in the carotid territory. Am J Neuroradiol. 1989;10:753-765.
26. Schumacher M, Schmidt D, Wakhloo A. Intra-arterial fibrinolytic therapy in central retinal artery occlusion. Neuroradiology. 1993;35:600-605.
27. Arnold M, Koerner U, Remonda L, et al. Comparison of intra-arterial thrombolysis with conventional treatment in patients with acute central retinal artery occlusion. J Neurol Neurosurg Psychiatry. 2005;76:196-199.
28. Aldrich EM, Lee AW, Chen CS, et al. Local intraarterial fibrinolysis administered in aliquots for the treatment of central retinal artery occlusion. Stroke. 2008;39:1746-1750.
29. Schumacher M, Schmidt D, Jurklies B, et al. Central retinal artery occlusion: local intra-arterial fibrinolysis versus conservative treatment, a multicenter randomized trial. Ophthalmology. 2010;117:1367-1375.
30. Pielen A, Patenburg S, Schmoor C, et al. Predictors of prognosis and treatment outcome in central retinal artery occlusion: local intra-arterial fibrinolysis vs. conservative treatment. Neuroradiology. 2015;57:1055-1062.
31. Hayreh SS. Comment re: multicenter study of the European Assessment Group for Lysis in the Eye (EAGLE) for the treatment of central retinal artery occlusion: design issues and implications. Graefes Arch Clin Exp Ophthalmol. 2007;245:464-466; author reply 467-470.
32. Anupriya A, Aaron S. Thrombolysis for artery occlusion. Ophthalmology. 2011;118:604.
33. Arruga J, Sanders MD. Ophthalmologic findings in 70 patients with evidence of retinal embolism. Ophthalmology. 1982;89:1336-1347.
34. Hattenback LO, Kuhli-Hattenback C, Scharrer I, Baatz H. Intravenous thrombolysis with low-dose recombinant tissue plasminogen activator in central retinal artery occlusion. Am J Ophthalmol. 2008;146:700-706.
35. Chen CS, Lee AW, Campbell B, et al. Efficacy of intravenous tissue-type plasminogen activator in central retinal artery occlusion. Stroke. 2011;42:2229-2234.
36. Schrag M, Youn T, Schindler J, et al. Intravenous fibrinolytic therapy in central retinal artery occlusion: a patient-level meta-analysis. JAMA Neurol. 2015;72:1148-1154.
37. Mazzeo F, Giorgi D, Cerutti F, et al. Giant cell arteritis: the importance of immediate and appropriate diagnosis and treatment for better prognosis. Clin Ophthalmol. 2012;6:909-913.
38. Mason JO 3rd, Patel SA, Feist RM, et al. Ocular neovascularization in eyes with a central retinal artery occlusion or branch retinal artery occlusion. Clin Ophthalmol. 2015;9:995-1000.
39. Rudkin AK, Lee AW, Chen CS. Ocular neovascularization following central retinal artery occlusion: prevalence and timing of onset. Eur J Ophthalmol. 2010;20:1042-1046.