







Management of Intraocular Foreign Bodies of the Posterior Segment
Treatment strategies to maximize anatomical and functional outcomes
ANDREW FRANCIS, MD • WILLIAM F. MIELER, MD
Open globe injury (OGI) repair remains one of the most challenging surgeries in all of ophthalmology. Intraocular foreign bodies (IOFBs) constitute a unique subset of OGIs with special treatment considerations.
To date, there are no prospective, randomized, double-blind, controlled trials to offer the trauma surgeon guidelines for the management of these serious, and often blinding, traumatic eye injuries. Complicating matters, the removal of posterior-segment IOFBs is often complicated by limited visibility from injury to the cornea or lens or dense vitreous hemorrhage, which must be managed effectively to ensure safe removal of the offending IOFB.
The patient’s very real concern regarding permanent vision loss mandates a compassionate, thoughtful plan to rehabilitate the damaged globe and to remove the IOFB. Several controversies exist in the management of IOFBs that will be reviewed in this article.
To maximize both anatomical and functional success, the surgeon must first and foremost gain the patient’s trust through effective communication, followed by the development of a strategic plan for repair of the injury, removal of the IOFB, and long-term rehabilitation, which may ultimately require additional surgeries with an uncertain prognosis.
Andrew Francis, MD, is a senior ophthalmology resident at the University of Illinois at Chicago and will begin a vitreoretinal surgical fellowship at the University of California at San Francisco in the summer of 2016. William F. Mieler is the Cless Family Professor in Ophthalmology at the University of Illinois at Chicago. They report no financial interests in products mentioned in this article. Dr. Mieler can be reached via e-mail at wmieler@uic.edu
The trauma specialist must always remember: “The physician-patient relationship is established by chance, not by choice: the trust of the patient, an absolutely integral part of an optimal physician-patient relationship, must be earned. Earning this trust is not easy, and ‘bedside manner’” (i.e., the act of counseling) exhibited by the ophthalmologist is as important in this process as are his treatment results.”1
EPIDEMIOLOGY
IOFBs account for 18% to 41% of all OGIs, with the vast majority of cases (>90%) occurring in young men between the ages of 29 and 38 years old.2-4 Work-related injuries are most common (54-72%) followed by injuries at home (30%). The most common mechanisms of injury include hammering metal on metal (60-80%), power tools (18-25%), and gunshots or explosives (19%).2
IOFBs are an especially common injury known to affect military service members exposed to improvised explosive devices (IEDs), especially in recent combat zones such as in Iraq or Afghanistan, accounting for up to 25% of all traumatic OGIs.5
PATHOPHYSIOLOGY
The extent of trauma from IOFBs is associated with the size, shape, speed, density, and velocity of the object, as well as the composition of the penetrating or perforating material.6 Very sharp, high-velocity projectiles result in less damage than blunt, low-velocity objects7 due to less transfer of energy from the smaller object through a smaller wound.
Corneal entry is also often associated with less damage than scleral entry for the same reason, along with a lessened risk of retinal injury. In addition, there is an inverse relationship between wound length and the occurrence of retinal damage.
High-risk features include organic matter contamination in a rural setting, development of endophthalmitis, and features such as a high percentage of copper in the offending material, which can result in an acute, inflammatory toxicosis that mimics endophthalmitis, with potentially dire consequences for the affected eye.
ASSESSMENT
A detailed history should be taken in all patients suspected of harboring an IOFB, with special consideration for the mechanism of injury, the setting in which the injury occurred, the date and time of the injury, the preoperative visual acuity, and whether eye protection was worn. In addition, an evaluation of systemic medical issues, medication allergies, time since the last meal, and any previous interventions should also be documented.
The vital question with any OGI that must be answered is whether an IOFB is present and, if it is, where is it located within the eye. Surprisingly, many patients may not report experiencing pain or a foreign body sensation after sustaining the injury, and they may be unable to recall the precipitating events leading to the suspected injury.
Under no circumstances can the physician afford to miss the presence of an IOFB because it can result in serious medical and legal consequences. If the patient history and the clinical suspicion of the ophthalmologist oppose one another, an IOFB must be assumed to be present and a rigorous search performed.
Clinical findings that raise the suspicion of an IOFB include, but are not limited to, a shallow anterior chamber, low intraocular pressure, Seidel-positive wounds, an irregular pupil, lens trauma, hyphema, iris transillumination defects, hemorrhagic chemosis, subconjunctival hemorrhage, uveal extrusion, restriction of extraocular motility, and an afferent pupillary defect.
In all cases of suspected IOFB, computed tomography imaging (preferably a helical spiral CT with 1.0-mm-thin cuts) of the orbits should be performed with scanning on both the sagittal and coronal planes.
Magnetic resonance imaging should only be employed when the presence of a metallic IOFB has been excluded by CT. Echography may also be employed, although the direct application of the probe onto the damaged globe risks distortion of the intraocular anatomy and possible extrusion of intraocular contents.
Tetanus vaccination should be updated, and prophylactic antibiotics are recommended, although the route of administration remains controversial. Anesthesia should be contacted to determine the availability of the operating room and whether general anesthesia is an option. The OR nursing staff should also be mobilized and special equipment made available for the planned procedure.
CONTROVERSIES IN MANAGEMENT
There are several unresolved issues in the management of IOFBs and OGI repair. Although a detailed discussion of each of these issues is beyond the scope of this article, several specific issues warrant further discussion. These include, but are not limited to, timing of the IOFB removal (early vs delayed intervention), the method and route of IOFB removal (internal surgical approach vs the use of an external magnet), the role of a prophylactic scleral buckle in an OGI, the benefit of or need for prophylactic antibiotics and their route of administration, and the placement of an intraocular lens in the acute traumatic setting.8
Timing of IOFB Removal
The timing of IOFB removal depends on several factors, including, but not limited to, the nature of the injury (mechanism, speed, mass, and volume of the offending object), the composition of the IOFB (metallic, high velocity “sterile” projectiles vs organic material, ferrous, copper, or inert materials, such as glass), the time since the injury occurred (part of a comprehensive history), and the general medical status of the patient (additional life-threatening injuries vs a patient in otherwise good health).
If the composition of the IOFB is unknown, but signs of inflammation are present, an immediate, rather than a delayed, approach should be undertaken. If the patient is otherwise stable, ophthalmologists with limited experience removing IOFBs may consider referral to specialists in their community who have more experience managing these complex injuries.
Because no prospective, randomized clinical trials have been performed on this subject, research has been limited to retrospective analyses. Advocates for removal within 24 hours cite the reduced incidence of endophthalmitis; however, these studies have not been of sufficient power to detect significant differences, they have usually lacked control groups, and they have often included a range of presenting VAs, intraocular IOFB presentations, various associated injuries to the globe and retina, and durations before wound closure occurred.9-12
Delays in wound closure and the IOFB material, in particular, are likely more significant risk factors for the development of post-traumatic endophthalmitis and poor visual outcomes than the presence of the IOFB itself.
Investigators arguing that the timing of IOFB removal is not a significant prognostic factor may cite several sources,5,13-17 which have described favorable outcomes in war settings even when the IOFB was removed one month later (as long as there was no infection).
These studies share many of the same concerns regarding design, patient selection, and absence of control groups as studies advocating for immediate surgery, although advocates of a delayed approach can also cite the possibly decreasing complexity of the procedure after several days following the initial injury, which is believed to allow for spontaneous separation of the posterior hyaloid face and liquefaction of traumatic blood clots, enabling easier removal by vitrectomy. In addition, a delayed approach may allow for the resolution of traumatic hyphema or fibrinoid aqueous and could allow for improved clearance of corneal edema.8
The finding of retained IOFBs many years after injury in otherwise asymptomatic patients is further evidence that IOFBs are not always harmful, although these patients should be followed up with serial ocular examinations, echography, visual evoked potentials, and electroretinography to monitor for possible further injury (especially with iron- and/or copper-containing IOFBs).
Surgical Technique
Pars plana vitrectomy is now the preferred method for the removal of IOFBs and repair of associated retinal injury.2,16,18-21 Historically, before the era of routine PPV, external electromagnets were the primary means of removing metallic IOFBs. Early IOFB removal was advocated to prevent encapsulation. These large, cumbersome devices were unpredictable and often resulted in serious iatrogenic injury to the globe and the development of proliferative vitreoretinopathy, with its associated complications.
Vitrectomy provides the best access for repairing concurrent retinal injury, including vitreous hemorrhage, retinal tears, detachments, and lenticular injury (Figure 1). Additionally, PPV has the advantage of large-volume irrigation of the posterior segment, which likely reduces the risk of postoperative endophthalmitis.
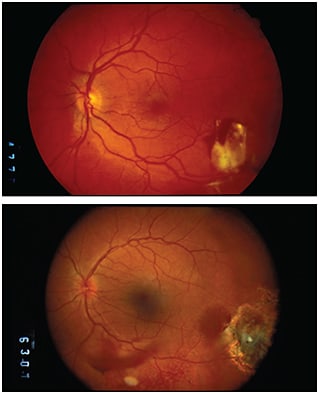
Figure 1. Top) Image of an intraretinal glass IOFB, with pre-operative VA of 20/40. The removal process involved a PPV, freeing of the encapsulated intraretinal glass IOFB, removal by forceps, and placement of endophotocoagulation around the margins of the IOFB removal site. Bottom) Postoperative image, showing removal of the IOFB, with laser demarcation around the previous retinal IOFB site. VA stabilized at 20/20.
Today, the routine application of PPV and the use of intraocular forceps and intraocular magnets (IOMs) have improved the prognosis for IOFB removal, and these patients tend to do better visually then those with other types of OGI.8,13,22,23
With modern vitrectomy techniques and the availability of IOMs and intraocular forceps, VA of 20/40 or better can be obtained in approximately 60% of patients.3,24-26 When the visual outcome is limited, it is generally the result of the effects of the initial injury or development of postoperative retinal detachment with PVR or hypotony.
Before starting the vitrectomy, an undiluted vitreous sample should be obtained for Gram staining and culture. Media opacities, including hyphema, cataract, and vitreous hemorrhage, should be removed. A standard three-port PPV system is used, with microincisional small-gauge surgery (23- or 25-gauge) performed routinely (with possible enlargement of one sclerotomy or the creation of a limbal opening to remove larger IOFBs).
The cortical vitreous is completely removed, and a posterior vitreous detachment is generally created. All vitreous adhesions in contact with the IOFB are then circumferentially removed until the IOFB is freed of all scar tissue. The IOFB is then removed either with an internal magnet or with forceps, depending upon the composition of the IOFB. An algorithm for IOFB extraction based on the size and material of the object is shown in Figure 2.
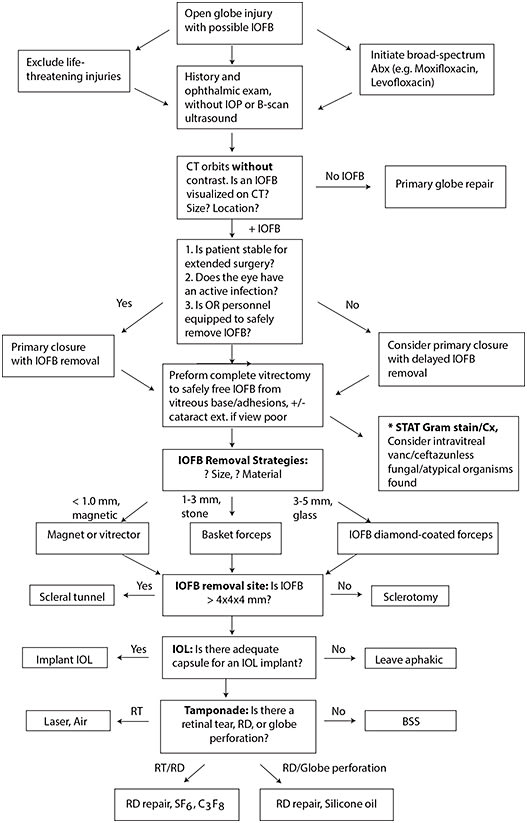
Figure 2. Algorithm for management of IOFBs after open globe injury.
ADAPTED FROM ORIGINAL, COURTESY OF WOLTERS KLUWER
Very small (<1.0 mm) ferromagnetic IOFBs can be removed with an IOM through a pars plana incision. Small metallic or nonmetallic IOFBs can be removed with the vitreous cutter. Intermediate-sized IOFBs (1.0 to 3.0 mm) can be removed with intraocular forceps (eg, de Juan) or basket forceps without regard to composition.
Large IOFBs (3.0 to 5.0 mm) and glass IOFBs may require a diamond-coated forceps designed to prevent slippage of the IOFB during removal or large foreign body forceps that open with active compression and close passively.21
Large-volume IOFBs (4.0 x 4.0 x 4.0 mm3 or greater) may require a scleral tunnel incision or be removed through a limbal wound, whereas small-volume IOFBs can be removed through the sclerotomy site with enlargement as needed in most cases.
Following IOFB removal, a detailed examination of the peripheral retina with scleral depression is performed to identify retinal tears, detachments, or choroidal detachments. Retinal tears are treated with endolaser, and the eye is filled with a long-acting gas (SF6 or C3F8) or silicone oil tamponade. Prophylactic cryotherapy is generally avoided due to the extensive inflammatory response that results from breakdown of the blood-retinal barrier, with an increased risk for PVR formation.8,27,28
The role of prophylactic scleral buckle placement after OGI either at the time of the initial surgery or later is controversial and is generally not indicated after routine IOFB removal. It may be useful in certain cases, including cases in which the scleral and retinal laceration extends posterior to the ora serrata and the peripheral retina cannot be completely visualized, to place a scleral buckle. However, further studies in this area are warranted to determine the true benefit.8,29
Following the completion of surgery, intravitreal antibiotics are often utilized. For endophthalmitis prophylaxis, intravitreal vancomycin (1.0 mg/0.1 mL) is routinely combined with intravitreal ceftazidime (2.25 mg/0.1 mL) for coverage of both Gram-positive and Gram-negative organisms, respectively. In patients with penicillin allergies, intravitreal amikacin (0.4 mg/0.1 mL), or occasionally moxifloxacin (100 µg/0.1 mL), may be substituted. Subconjunctival antibiotics may also be considered.11
Upon discharge, the patient is prescribed postoperative topical and oral antibiotics with fourth-generation fluoroquinolones, which have demonstrated excellent ocular penetration in this scenario.30,31
POSTOPERATIVE CARE AND COMPLICATIONS
The primary complications with prognostic significance following IOFB removal include postoperative endophthalmitis, postoperative retinal detachment, development of PVR, and hypotony. The risk of sympathetic ophthalmia, although rare, with an incidence between 0.28% and 1.9% of eyes, should always be considered in cases of unexplained, persistent postoperative granulomatous inflammation.32
Postoperative endophthalmitis is managed with aggressive topical and systemic antibiotics, with an early return to the OR for repeat PPV surgery with intravitreal antibiotic injection. Postoperative retinal detachment rates vary from 6% to 40% in the literature and are a common cause of poor functional outcomes.12,17,20,33-36 The early identification of this complication can be mitigated by emphasizing the importance of close postoperative follow-up and adherence to postoperative antibiotic medications.
Retinal detachment with PVR is a serious complication following IOFB removal, ranging from 7% to 46% in the literature, and it is a leading cause of secondary retinal detachment after PPV surgery.4,9,34,35,37 Risk factors associated with the development of PVR include the extent of intraocular injury, the number of retinal tears, presence of vitreous hemorrhage, a long, posteriorly located wound, persistent intraocular inflammation, and the size of the IOFB.17,21,38,39
FUTURE INNOVATIONS
Small-gauge (23-, 25-, and 27-gauge) PPV instruments, transconjunctival sutureless vitrectomy, and vitrectomy cutters with cut rates exceeding 5,000 cuts/min offer the vitreoretinal surgeon new technologies to approach the management of OGI with IOFBs.40
A theoretical benefit of these smaller vitrectomy instruments is improved access to intraocular spaces otherwise inaccessible with larger instruments. A disadvantage is that larger IOFBs will still require enlargement of the sclerotomies or a limbal approach to facilitate removal (as noted previously). Combining the use of these instruments with chandelier xenon light sources allows the vitreoretinal surgeon to apply a bimanual technique, obviating the need for an assistant in many cases.
Wide-angle binocular indirect ophthalmoscope viewing systems also improve the vitreoretinal surgeon’s visibility of extreme anterior retinal pathology and posterior-segment pathology through small pupils, avoiding the need for temporary keratoplasty in many cases.
CONCLUSION
The treatment and management of OGIs with IOFBs remain among the most formidable surgeries in all of ophthalmology. The inherent difficulties are numerous, but the potential rewards for the ophthalmic surgeon, and most importantly the patient, are vast.
Several controversies persist despite decades of experience, and these will likely continue into the foreseeable future given the lack of prospective studies and clinical trials. More than any other surgery in ophthalmology, uncertainty dominates the landscape, but with advances in vitreoretinal technology and the continued efforts of experienced surgeons to train the next generation of residents and fellows in the art of open globe injury repair and IOFB removal, there is hope for improved anatomical and functional outcomes in this unique population of vulnerable patients.
We close with a guiding principle for surgeons in training: “The surgeon can restore anatomy only; functional recovery always follows the anatomical one, and while anatomical reconstruction may be promised to the patient in many cases, the promise of functional improvement should not be given lightheartedly: whether anatomical restoration indeed brings improved function is a more complex issue with several unknowns.”1
REFERENCES
1. Kuhn F. Ocular Traumatology. Springer; Berlin, Germany; 2008.
2. Greven CM, Engelbrecht NE, Slusher MM, Nagy SS. Intraocular foreign bodies: management, prognostic factors, and visual outcomes. Ophthalmology. 2000;107:608-612.
3. Roper-Hall MJ. Review of 555 cases of intra-ocular foreign body with special reference to prognosis. Br J Ophthalmol. 1954;38:65-99.
4. Williams DF, Mieler WF, Abrams GW. Intraocular foreign bodies in young people. Retina. 1990;10(Suppl 1):S45-S49.
5. Colyer MH, Weber ED, Weichel ED, et al. Delayed intraocular foreign body removal without endophthalmitis during Operations Iraqi Freedom and Enduring Freedom. Ophthalmology. 2007;114:1439-1447.
6. Potts AM, Distler JA. Shape factor in the penetration of intraocular foreign bodies. Am J Ophthalmol. 1985;100:183-187.
7. Woodcock MG, Scott RA, Huntbach J, Kirkby GR. Mass and shape as factors in intraocular foreign body injuries. Ophthalmology. 2006;113:2262-2269.
8. Mittra RA, Mieler WF. Controversies in the management of open-globe injuries involving the posterior segment. Surv Ophthalmol. 1999;44:215-225.
9. Jonas JB, Knorr HL, Budde WM. Prognostic factors in ocular injuries caused by intraocular or retrobulbar foreign bodies. Ophthalmology. 2000;107:823-828.
10. Chaudhry IA, Shamsi FA, Al-Harthi E, Al-Theeb A, Elzaridi E, Riley FC. Incidence and visual outcome of endophthalmitis associated with intraocular foreign bodies. Graefes Arch Clin Exp Ophthalmol. 2008;246:181-186.
11. Mieler WF, Ellis MK, Williams DF, Han DP. Retained intraocular foreign bodies and endophthalmitis. Ophthalmology. 1990;97:1532-1538.
12. De Souza S, Howcroft MJ. Management of posterior segment intraocular foreign bodies: 14 years’ experience. Can J Ophthalmol. 1999;34:23-29.
13. Camacho H, Mejía LF. Extraction of intraocular foreign bodies by pars plana vitrectomy. A retrospective study. Ophthalmologica. 1991;202:173-179.
14. El-Asrar AM, Al-Amro SA, Khan NM, Kangave D. Visual outcome and prognostic factors after vitrectomy for posterior segment foreign bodies. Eur J Ophthalmol. 2000;10:304-311.
15. Karel I, Diblík P. Management of posterior segment foreign bodies and long-term results. Eur J Ophthalmol. 1995;5:113-118.
16. Mester V, Kuhn F. Ferrous intraocular foreign bodies retained in the posterior segment: management options and results. Int Ophthalmol. 1998;22:355-362.
17. Wickham L, Xing W, Bunce C, Sullivan P. Outcomes of surgery for posterior segment intraocular foreign bodies--a retrospective review of 17 years of clinical experience. Graefes Arch Clin Exp Ophthalmol. 2006;244:1620-1626.
18. Demircan N, Soylu M, Yagmur M, Akkaya H, Ozcan AA, Varinli I. Pars plana vitrectomy in ocular injury with intraocular foreign body. J Trauma. 2005;59:1216-1218.
19. Peyman GA, Raichand M, Goldberg MF, Brown S. Vitrectomy in the management of intraocular foreign bodies and their complications. Br J Ophthalmol. 1980;64:476-482.
20. Wani VB, Al-Ajmi M, Thalib L, et al. Vitrectomy for posterior segment intraocular foreign bodies: visual results and prognostic factors. Retina. 2003;23:654-660.
21. Yeh S, Colyer MH, Weichel ED. Current trends in the management of intraocular foreign bodies. Curr Opin Ophthalmol. 2008;19:225-233.
22. Kuhn F, Kovacs B. Management of postequatorial magnetic intraretinal foreign bodies. Int Ophthalmol. 1989;13:321-325.
23. Ahmadieh H, Sajjadi H, Azarmina M, Soheilian M, Baharivand N. Surgical management of intraretinal foreign bodies. Retina. 1994;14:397-403.
24. Johnston S. Perforating eye injuries: a five year survey. Trans Ophthalmol Soc U K. 1971;91:895-921.
25. Percival SP. A decade of intraocular foreign bodies. Br J Ophthalmol. 1972;56:454-461.
26. Percival SP. Late complications from posterior segment intraocular foreign bodies with particular reference to retinal detachment. Br J Ophthalmol. 1972;56:462-468.
27. Jaccoma EH, Conway BP, Campochiaro PA. Cryotherapy causes extensive breakdown of the blood-retinal barrier. A comparison with argon laser photocoagulation. Arch Ophthalmol. 1985;103:1728-1730.
28. Campochiaro PA, Kaden IH, Vidaurri-Leal J, Glaser BM. Cryotherapy enhances intravitreal dispersion of viable retinal pigment epithelial cells. Arch Ophthalmol. 1985;103:434-436.
29. Breit SM, Hariprasad SM, Mieler WF, Shah GK, Mills MD, Grand MG. Management of endogenous fungal endophthalmitis with voriconazole and caspofungin. Am J Ophthalmol. 2005;139:135-140.
30. Ahmed S, Kuruvilla O, Yee DC, et al. Intraocular penetration of systemic antibiotics in eyes with penetrating ocular injury. J Ocul Pharmacol Ther. 2014;30:823-830.
31. Mather R, Karenchak LM, Romanowski EG, Kowalski RP. Fourth generation fluoroquinolones: new weapons in the arsenal of ophthalmic antibiotics. Am J Ophthalmol. 2002;133:463-466.
32. Ozbek Z, Arikan G, Yaman A, Oner H, Bajin MS, Saatci AO. Sympathetic ophthalmia following vitreoretinal surgery. Int Ophthalmol. 2010;30:221-227.
33. El-Asrar AM, Al-Amro SA, Khan NM, Kangave D. Retinal detachment after posterior segment intraocular foreign body injuries. Int Ophthalmol. 1998;22:369-375.
34. Chiquet C, Zech JC, Gain P, Adeleine P, Trepsat C. Visual outcome and prognostic factors after magnetic extraction of posterior segment foreign bodies in 40 cases. Br J Ophthalmol. 1998;82:801-806.
35. Chiquet C, Gain P, Zech JC, Adeleine P, Denis P. [Risk factors for secondary retinal detachment after extraction of intraocular foreign bodies]. Can J Ophthalmol. 2002;37:168-176. French.
36. Soheilian M, Feghi M, Yazdani S, et al. Surgical management of non-metallic and non-magnetic metallic intraocular foreign bodies. Ophthalmic Surg Lasers Imaging. 2005 May-Jun 2005;36:189-196.
37. Chow DR, Garretson BR, Kuczynski B, et al. External versus internal approach to the removal of metallic intraocular foreign bodies. Retina. 2000;20:364-369.
38. Szijártó Z, Gaál V, Kovács B, Kuhn F. Prognosis of penetrating eye injuries with posterior segment intraocular foreign body. Graefes Arch Clin Exp Ophthalmol. 2008;246:161-165.
39. Cardillo JA, Stout JT, LaBree L, et al. Post-traumatic proliferative vitreoretinopathy. The epidemiologic profile, onset, risk factors, and visual outcome. Ophthalmology. 1997;104:1166-1173.
40. Fine HF, Iranmanesh R, Iturralde D, Spaide RF. Outcomes of 77 consecutive cases of 23-gauge transconjunctival vitrectomy surgery for posterior segment disease. Ophthalmology. 2007;114:1197-1200.