







Gore-Tex Sutured Intraocular Lens
A beginner’s guide for scleral fixation of posterior-chamber IOLs
EHSAN RAHIMY, MD • M. ALI KHAN, MD • OMESH P. GUPTA, MD • JASON HSU, MD
In the setting of inadequate capsular support, surgical options for intraocular lens placement include: (1) insertion of an anterior-chamber IOL; (2) iris fixation of a posterior-chamber IOL (PCIOL); and (3) scleral fixation (with or without suture) of a PCIOL.
The choice of technique is often influenced by the patient’s age, anatomical considerations (ie, prior trauma with iris tissue loss), other ocular comorbidities (ie, glaucoma), and ultimately, surgeon preference, as well as comfort level.
With regard to scleral fixated sutured IOLs, two different approaches have been described: an ab externo (outside-in) or an ab interno (inside-out) technique. In 2014, our institution described a modified ab externo method for two-point scleral fixation of a CZ70BD (Alcon, Fort Worth, TX) IOL using Gore-Tex (W.L. Gore & Associates, Newark, DE), a nonabsorbable polytetrafluoroethylene (PTFE) monofilament suture (Figure 1).1 This procedure was adapted from an earlier description by Slade et al2 and was modified to include concurrent 23-gauge pars plana vitrectomy.
Figure 1. Gore-Tex, a non-absorbable, polytetrafluoroethylene monofilament suture with greater tensile strength than polypropylene (Prolene, Ethicon, Inc., Somerville, NJ).
While traditionally used in cardiac and vascular surgery, Gore-Tex has been gaining popularity in ophthalmology because the resilient PTFE material may be less prone to suture breakage than the rate commonly encountered with polypropylene (Prolene, Ethicon, Inc., Somerville, NJ).3-5
With increased utilization and experience, this technique has recently undergone further modification. Chief among the adjustments made is the currently preferred use of an Akreos AO60 IOL (Bausch + Lomb, Rochester, NY), with a four-haptic design that enables excellent IOL centration and stabilization through four-point fixation (Figure 2).
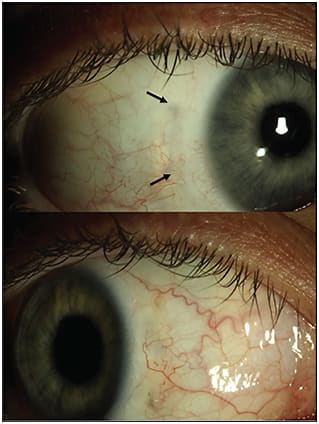
Figure 2. Postoperative outcome demonstrating four-point fixation of an Akreos AO60 intraocular lens with an excellent cosmetic and functional result. Arrows indicate previous temporal sclerotomy sites with an externalized loop of Gore-Tex suture in between.
Although any of the aforementioned strategies can be employed effectively in aphakia with poor capsular support, we believe that scleral fixation of an Akreos AO60 IOL with Gore-Tex suture has numerous advantages, including relative ease of insertion and fixation through small corneal incisions, minimized IOL tilt, avoidance of iris contact, and a theoretically lower risk of lens dislocation.
This article presents a brief overview of the salient steps of the procedure, along with situational considerations and helpful tips for achieving the best results.
Ehsan Rahimy, MD, is a vitreoretinal specialist at the Palo Alto Medical Foundation in Palo Alto, CA. M. Ali Khan, MD, is a vitreoretinal fellow at the Wills Eye Institute in Philadelphia, PA Omesh P. Gupta, MD, and Jason Hsu, MD, serve on the faculty of Wills. None of the authors reports any financial interest in any of the products mentioned here. Dr. Rahimy can be reached via e-mail at rahimye@pamf.org.
SURGICAL TECHNIQUE
The key steps to this procedure are outlined in Video 1 (online). Beginning at the horizontal meridian, limited superonasal and inferotemporal 90° conjunctival limbal peritomies are created with relaxing radial incisions. External cautery is used to obtain hemostasis. Next, a standard infusion line for PPV is introduced (typically inferiorly or in the inferonasal quadrant, away from the sclerotomies for suture fixation maneuvers).
A toric lens marker is then used to mark the corneal limbus at two points on the horizontal plane, 180° apart. The two cannulas are then placed in this axis 3 mm posterior to the limbus. The introducer is then used to construct two additional sclerotomies: one 5 mm inferotemporal to the temporal cannula; and the second 5 mm superonasal to the nasal cannula, while maintaining a 3-mm displacement from the limbus (Figure 3A).
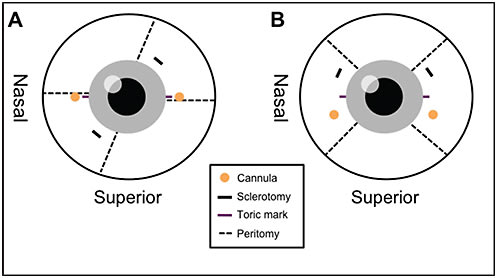
Figure 3. Two different schematics for placement of the conjunctival peritomies and sclerotomies when performing a Gore-Tex sutured intraocular lens procedure.
Note that all scleral incisions are made with a straight-entry, nontunneled approach and with the flat portion of the trocar blade parallel to the limbus. Standard PPV can then be performed. This technique is compatible with 23-, 25-, or 27-gauge instrumentation.
The anterior chamber may be then entered either through a previously created clear corneal incision (if recent cataract extraction was performed) or by constructing a new incision through the superior cornea using a 2.75-mm phaco keratome blade. The internal lip of the scleral wound can be slightly enlarged to 3.5-4.0 mm. With the infusion clamped, the corneal endothelium is stabilized using intracameral viscoelastic.
Next, the CV-8 needles of the 8-0 Gore-Tex suture are amputated, and the suture is cut into two halves. Each suture end is then threaded through two adjacent eyelets of the Akreos AO60 lens at equal lengths for eventual four-point fixation of the IOL inside the eye.
To minimize the potential for iris chafing, the suture is passed through the first eyelet in an anterior to posterior fashion and then from posterior to anterior as it exits through the corresponding second eyelet. This pattern is repeated with the second half of the suture on the contralateral side of the IOL.
In a hand-to-hand technique, either the nasal or temporal two ends of the Gore-Tex suture are passed into the anterior chamber and pulled out of each corresponding sclerotomy using flat intraocular forceps (eg, Alcon MaxGrip forceps).
The Akreos AO60 IOL can then be folded along its long axis using Kelman-McPherson or similar forceps and introduced into the anterior chamber. Once in the eye, the IOL is displaced into the posterior chamber, and under direct visualization, the two trailing nasal/temporal ends of the Gore-Tex suture can be grasped and externalized through the respective sclerotomies using intraocular forceps. All four ends of the Gore-Tex suture are then pulled, and tension is balanced to ensure that the IOL optic is well centered.
The trocars are then individually removed over the Gore-Tex, and the sutures are tied using either a 3-1-1 or adjustable slipknot technique. The knots are trimmed and buried into the sclerotomies that previously housed the cannulas to minimize the chance of wound leakage because these incisions tend to be more dilated.
The viscoelastic material is then irrigated out of the anterior chamber, and the corneal wound may be closed using a 10-0 Nylon suture. The overlying conjunctival peritomy is then closed, ensuring that the externalized loop of the Gore-Tex suture is completely covered.
TEN HELPFUL TIPS AND TRICKS
Beginning users unfamiliar with this technique tend to have questions regarding the execution of certain intraoperative steps, as well as perioperative considerations when planning whether and for whom this procedure may be a viable alternative to traditional secondary IOL methods. We have included the following tips to help troubleshoot and optimize surgical outcomes.
1. Preoperative Conjunctival Assessment
The relative ease, or difficulty, of handling the conjunctiva (especially closure at the end of the case) can make all of the difference in the case length, as well as the surgeon’s perceived difficulty of the procedure.
An important consideration is whether the patient has had previous ocular surgery in which the conjunctiva was manipulated. Is there a history of prior scleral buckling? Have there been multiple vitrectomies? Has the patient undergone a glaucoma filtration procedure with trabeculectomy or tube shunt?
It is important not to overlook such a history because these patients may fit the demographic potentially in need of a secondary IOL (ie, prior retinal detachment that underwent scleral buckle, PPV, and lensectomy, or a patient with glaucoma and filtering bleb now needing a secondary IOL in which an anterior-chamber lens would be preferably avoided). Such eyes may not be ideal candidates for a surgeon’s initial experience attempting this technique.
In limited cases in which the conjunctiva was too friable to adequately cover the exposed loop of Gore-Tex, we have had success using a Tutoplast (IOP Ophthalmics, Costa Mesa, CA) scleral patch graft to cover the suture.
2. Incision Planning
Based on certain anatomical considerations, the surgeon may consider rotating the placement of the conjunctival peritomies and sclerotomies to better facilitate subsequent intraocular maneuvers. We have popularized two different schemes that are outlined in Figure 3.
In situations in which the cataract surgeon created a superior corneal incision, a superior approach in which the four sclerotomies straddle the horizontal meridian (2 mm superior and inferior to the toric markings) with the cannulas housed in the superior sclerotomies may be preferred (Figure 3B).
Alternatively, in a patient with a prominent nasal bridge, the surgeon may have difficulty executing certain maneuvers with the intraocular forceps. In such instances, it may be more convenient for the surgeon to create the initial conjunctival peritomies in the superonasal and inferotemporal quadrants. While the cannulas are still inserted 180° apart in the horizontal meridian in line with the toric markings, the supplemental sclerotomies are created 4 mm superonasal to the nasal cannula and 4 mm inferotemporal to the temporal cannulas (Figure 3A). This maneuver effectively shifts the axis of IOL fixation away from the nasal bridge, creating more operating space for the surgeon.
Furthermore, when disposable intraocular forceps are being used (eg, Alcon MaxGrip forceps), the shaft can be bent to assume a curvilinear configuration for easier manipulation when working through the nasal sclerotomies.
3. How Many Millimeters From the Limbus?
The decision to place the sclerotomies 2.0 or 3.0 mm from the limbus is surgeon dependent. Anecdotally, we have observed that IOL placement 2.0 mm posterior to the limbus can occasionally result in contact with the posterior iris in select cases (both intraoperatively, using endoscopic visualization, and postoperatively, using ultrasound biomicroscopy).
For this reason, most surgeons at our institution have adjusted their sclerotomy placement to 3.0 mm posterior to the limbus. Accordingly, the desired IOL power becomes equivalent to an “in-the-bag” placement of the lens. If the surgeon elects to create sclerotomies 2.0 mm from the limbus, the IOL calculation should then be adjusted for a sulcus-placed lens (Figure 4).
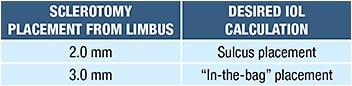
Figure 4. Adjustment of desired intraocular lens power based on sclerotomy distance from the limbus.
4. Extent of Vitrectomy Needed
Given that some of these patients may be young with an intact posterior hyaloid, the surgeon may encounter a decision regarding how thorough a vitrectomy to perform. In instances in which a posterior vitreous detachment is not present, we would recommend proceeding cautiously and only performing a thorough anterior and core vitrectomy to clear as much vitreous gel away from the eventual position of the Akreos AO60 IOL as possible. The reason for this would be to avoid iatrogenic retinal breaks during PVD induction, which may then necessitate use of an intraocular tamponade agent (see Tip #9: Use of intraocular air or gas).
5. Being Mindful of the Iris
Avoid excessive manipulation of iris tissue because it can contribute to progressive pupillary constriction throughout the course of the case, creating difficulty during the critical latter steps in which confirmation of correct suture and haptic orientation in the eye are dependent upon a permissible view.
Particularly in cases in which poor pupillary dilation may be an issue from the onset of the case (eg, pseudoexfoliation syndrome), the surgeon may consider preemptively using iris hooks to optimize the view.
Furthermore, good corneal wound construction, combined with being cognizant of when to clamp the infusion line, helps to minimize the risk of iris prolapse through the corneal wound, which can result in a suboptimal cosmetic result with patchy areas of iris atrophy and an irregular, eccentric pupil.
6. Management of Suture Ends
The surgeon should keep meticulous track of the suture ends both within and outside the eye to minimize confusion, which can result in tangling the sutures and twisting the IOL. We recommend placing the two nasal or two temporal ends of the Gore-Tex suture into the anterior chamber first and externalizing them through the sclerotomy sites prior to placing the IOL into the anterior chamber (Figure 5). This choice minimizes the number of free suture ends within the eye after placement of the IOL.
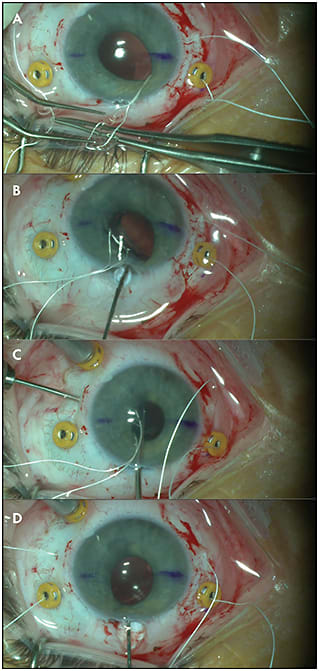
Figure 5. When managing suture ends, it is helpful to place either the two nasal or two temporal ends of the Gore-Tex suture into the anterior chamber and externalize them through their sclerotomy sites first before placing the intraocular lens (IOL) into the anterior chamber (A). This minimizes the number of free suture ends within the eye after placement of the IOL. After the IOL has been displaced posteriorly into the ciliary sulcus (B), the remaining two sutures can then be passed into the eye and externalized through their respective sclerotomies (C and D).
Next, it is helpful to use a Lester pusher (or similar instrument) to push the IOL to one side for direct visualization of the trailing Gore-Tex suture ends as they come out of the eyelets. The forceps can then be used to grasp the suture and pull it out through each of the remaining two sclerotomies, which will ensure that the correct suture has been pulled through and will further minimize the likelihood of tangling or pulling the wrong suture.
7. IOL Centration
The suture ends should not be tied so firmly as to create a “bowing” effect of the haptics on the lens. It is helpful to first center the IOL and then to incrementally adjust the suture tension on the nasal and temporal ends prior to tying a permanent knot. An adjustable slipknot may be helpful in this regard. Prior to locking the knots, a Lester or Sinskey hook can be used to displace the iris and visualize the peripheral eyelets to ensure that the suture is taut, without any crimping of the haptics.
8. Tying and Trimming Gore-Tex
Whether the surgeon uses a 3-1-1 or adjustable slipknot method to tie the suture, we recommend leaving a sufficient tail when trimming the suture, which can theoretically help decrease the risk of the Gore-Tex suture unraveling in the future. The surgeon might additionally consider rotating and burying the knot into the eye first before trimming the suture.
9. Use of Intraocular Air or Gas
Previous reports have noted opacification of hydrophilic acrylic IOLs, including the Akreos AO60, with concurrent use of intraocular air during Descemet stripping endothelial keratoplasty.6 Caution must be taken if air or gas is required for a vitreoretinal surgery indication. The patient should be counseled accordingly that, if such a tamponade agent is needed, there is a rare chance of IOL opacification, in which case the lens might need to be exchanged.
10. Wound Closure
Particularly in the setting of an extensive vitrectomy, the sclerotomies may leak at the conclusion of the case (especially those that housed the cannulas). To avoid postoperative hypotony, leaking sclerotomy sites can be sutured with 6-0 plain gut or 8-0 polyglactin 910 (Vicryl, Ethicon) sutures.
Care should be taken not to cut the Gore-Tex suture that has been already passed through the sclerotomy. This step can be performed by suturing through the corner of the sclerotomy away from where the Gore-Tex suture is hugging. In our experience, using 27-gauge instrumentation may decrease the risk of sclerotomy leakage requiring suture placement at the conclusion of the case (Video 2, online).7
SURGICAL OUTCOMES
A retrospective series from our institution of 85 eyes undergoing ab externo IOL scleral fixation with Gore-Tex sutures across varying indications was recently published in 2015.8 Over a mean follow-up period of 325 days, logMAR visual acuity improved from 1.43 ± 0.72 (Snellen equivalent, 20/538) preoperatively to 0.64 ± 0.61 (Snellen equivalent, 20/87) postoperatively (P<.001).
No intraoperative complications were encountered. In the postoperative period, transient hypotony, believed to be secondary to incompetence of 23-gauge wounds, was the most commonly observed adverse event, occurring in eight eyes (9.4%). In all instances, the hypotony resolved by postoperative day 30 without any further intervention.
No suture-related complications, including breakage, erosion, IOL dislocation, IOL tilt, endophthalmitis, or persistent postoperative inflammation, were encountered during the follow-up period.
RESCUE OF DISLOCATED IOLS
There are limited reports in the literature describing techniques for refixation of a previously scleral-sutured IOL that has subsequently dislocated. Breakage of polypropylene sutures can occur secondary to knot erosion, suture degradation, or iatrogenic severing of the suture by contact with the lens haptic.
In a histopathological assessment, Parekh et al4 reported that cutting of the suture by the sharp haptic surface was the most likely etiology for lens dislocation. In a series by Kim et al,9 trauma and an underlying diagnosis of Marfan syndrome were associated with an increased incidence of lens dislocation after previous IOL scleral fixation.
In our experience, many of the same principles described herein with Gore-Tex sutured IOL fixation can be successfully utilized to rescue a dislocated IOL (Video 3, ). The best candidates for this rescue procedure would be patients in whom the dislocated IOL contains an eyelet (ie, CZ70BD). Being able to refixate such lenses helps to avert explantation and exchange of the lens, significantly reducing the operating time and potential case complexity.
CONCLUSIONS
Ab externo scleral fixation of an Akreos AO60 IOL with Gore-Tex suture can be efficiently performed by vitreoretinal surgeons in conjunction with standard PPV. In our cumulative clinical experience, the technique is not technically difficult to master, it can be performed in a time-efficient manner, and it results in favorable visual outcomes with low rates of intraoperative and postoperative complications.
Formal evaluation of postoperative IOL position using imaging modalities, such as ultrasound biomicroscopy and anterior-segment optical coherence tomography, is ongoing. Despite these encouraging early findings, long-term outcomes of at least five, if not 10, years are needed to more definitively characterize the advantages and any potential disadvantages of using this technique. RP
REFERENCES
1. Khan MA, Gerstenblith AT, Dollin ML, et al. Scleral fixation of posterior chamber intraocular lenses using Gore-Tex suture with concurrent 23-gauge pars plana vitrectomy. Retina. 2014;34:1477-1480.
2. Slade DS, Hater MA, Cionni RJ, Crandall AS. Ab externo scleral fixation of intraocular lens. J Cataract Refract Surg. 2012;38:1316-1321.
3. Price MO, Price FW Jr, Werner L, Berlie C, Mamalis N. Late dislocation of scleral-sutured posterior chamber intraocular lenses. J Cataract Refract Surg. 2005;31:1320-1326.
4. Parekh P, Green WR, Stark WJ, Akpek EK. Subluxation of suture-fixated posterior chamber intraocular lenses a clinicopathologic study. Ophthalmology. 2007;114:232-237.
5. Drews RC. Polypropylene in the human eye. J Am Intraocular Implant Soc. 1983;9:137-142.
6. Werner L, Wilbanks G, Nieuwendaal CP, et al. Localized opacification of hydrophilic acrylic intraocular lenses after procedures using intracameral injection of air or gas. J Cataract Refract Surg. 2015;41:199-207.
7. Khan MA, Rahimy E, Gupta O, Hsu J. Combined 27-gauge pars plana vitrectomy and scleral fixation of an Akreos AO60 intraocular lens using Gore-Tex® suture. Under review for publication.
8. Khan MA, Gupta OP, Smith RG, et al. Scleral-fixation of intraocular lenses using Gore-Tex® suture: clinical outcomes and safety profile. Br J Ophthalmol. 2015 Aug 15. [Epub ahead of print]
9. Kim J, Kinyoun JL, Saperstein DA, et al. Subluxation of a transcleral sutured posterior chamber intraocular lens. Am J Ophthalmol. 2003;136:382-384.