







Anti-VEGF Agents in ROP
Finding balance between efficacy and adverse events
VISHAK J. JOHN, MD • CLAUDIA G. HOOTEN, MD • NICK GRISSOM, BS
Retinopathy of prematurity (ROP) is a vasoproliferative retinal disorder that can lead to significant blindness in children, especially in developing countries. It is mainly associated with early gestational age (<30 weeks of gestation) and low birth weight (≤1,500 g). Vision loss occurs secondary to vitreous hemorrhage, macular dragging, and retinal detachment.1
The pathogenesis of ROP consists of an initial phase of low VEGF levels and lack of vessels, followed by a phase of high VEGF levels and vessel proliferation.2-5 In embryology, the retina does not fully vascularize until 36 weeks nasally and at 40 weeks temporally. Premature infants are born into a high oxygen environment that leads to downregulation in retinal vascularization, leading to avascular peripheral retina.
Then, as the infant continues to grow, the avascular retina exists in a state of hypoxia, leading to neovascularization (Figure 1).2-4 Over the past several decades, research has demonstrated this association, and treatment has been directed toward minimizing the factors stimulating vessel proliferation.6,7
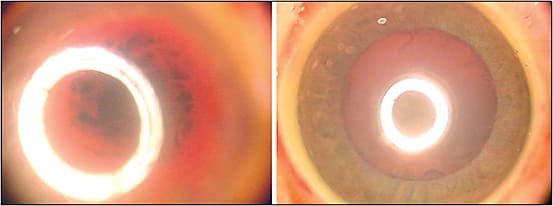
Figure 1. Iris neovascularization limiting dilation and view in a premature baby; right image is one week after bevacizumab injection.
ALL IMAGES APPEAR COURTESY OF AUDINA BERROCAL, MD
THE TREATMENT LANDSCAPE
Randomized, controlled trials have helped to transform the treatment of ROP.
The Cryotherapy for Retinopathy of Prematurity (CRYOROP) study, published in 1988, established the benefit of peripheral retinal ablation for threshold ROP. At 15 years, there was a decrease of >40% in unfavorable structural outcomes and a decrease of 30% in unfavorable visual acuity in treated eyes, compared with untreated eyes.
Vishak J. John, MD, is assistant professor in the Department of Ophthalmology at Wake Forest Baptist Medical Center in Winston-Salem, NC. Claudia G. Hooten, MD, is a retina fellow at Wake Forest. Nick Grissom, BS, is a medical student at Wake Forest. None of the authors report any financial interests in any products mentioned in this article. Dr. John can be reached via e-mail at vjohn@wakehealth.edu.
CRYOROP was also important in creating neonatal screening for acute ROP.8 The Early Treatment of Retinopathy of Prematurity (ETROP) study followed and demonstrated a benefit in earlier laser treatment compared to conventional management.9
Ablation therapy has its disadvantages, including corneal edema, inflammation, cataract formation, intraocular hemorrhage, anterior-segment ischemia, synechiae, and intraocular pressure changes. In the long term, these complications can lead to permanent loss of peripheral vision, glaucoma, strabismus, and severe myopia.
Geloneck et al described the increased presence of very high myopia in the laser group vs the bevacizumab (Avastin, Genentech, South San Francisco, CA) group at mean age of 2.5 years old among the patients in the Bevacizumab Eliminates the Angiogenic Threat of Retinopathy of Prematurity (BEAT-ROP) study (Figure 2).

Figure 2. Preparation of the eye with a speculum and povidone-iodine in the NICU for intravitreal bevacizumab injection.
Spherical equivalent refractions in patients with zone 1 had an average myopia of -1.51 D in the bevacizumab group compared to -8.44 D in the laser group, and neonates with posterior zone 2 disease were on average -0.58 D in the bevacizumab group compared to -5.83 D in the laser group.10
In addition, most clinicians intubate premature infants to perform laser treatment, thus carrying the risks of the adverse effects of anesthesia. Modern studies have also demonstrated that disease may progress even after appropriate surgical treatment with laser, thus suggesting the need for additional therapeutic options.11
Additionally, some patients with aggressive posterior ROP will continue to have poor outcomes after photocoagulation.12 Therefore, anti-VEGF agents have entered the clinical realm to address this problem.
THE EMERGING ROLE OF INTRAVITREAL ANTI-VEGF AGENTS
VEGF plays a significant role in angiogenic pathologies.5,6 Bevacizumab was FDA approved in 2004 to treat metastatic colorectal cancer, and it subsequently emerged for the treatment of neovascular retinal disorders, such as exudative age-related macular degeneration, and diabetic and retinal occlusive diseases.
Intravitreal injections of anti-VEGF molecules such as bevacizumab and ranibizumab (Lucentis, Genentech) have been demonstrated to diminish the neovascular response in animal models of ROP, and randomized, clinical trials have demonstrated their benefit in ROP in humans.
In the last decade, three randomized, controlled clinical trials and numerous case series have demonstrated the value of the off-label use of intravitreal bevacizumab and ranibizumab for ROP. A systematic analysis in 2014 of the off-label use of bevacizumab and ranibizumab revealed more than 50 studies documenting the outcomes of anti-VEGF treatment for ROP, and additional studies have been published since that time.13
In 2009, Micieli et al published a case series 14 eyes of 10 patients that were treated mainly for zone 1 and posterior zone 2 disease. Favorable outcomes were seen in 11 of 14 cases after treatment with bevacizumab.14
Lalwani and colleagues found bevacizumab helpful as a rescue treatment in progressive threshold ROP after prior laser treatment.15 In 2009, Law et al also replicated the use of bevacizumab as an adjunctive treatment for ROP in 13 patients who demonstrated regression of anterior vascular activity and improved pupillary dilation.16
BEAT-ROP AND BEYOND
The BEAT-ROP study was published in 2011, revolutionizing the role of bevacizumab for the treatment of ROP. This was the first randomized, prospective, multicenter, controlled trial that compared conventional laser to intravitreal bevacizumab. The primary outcome was recurrence of ROP in one or both eyes requiring retreatment before 54 weeks of postmenstrual age. The study showed a significant benefit of bevacizumab for zone 1 but not zone 2 disease with stage 3 plus ROP.
Furthermore, Mintz-Hittner et al showed that development of peripheral retinal vascularization continued in bevacizumab-treated eyes, which was not seen in the laser group.1 The trial was too small to assess safety (Figure 3, page 48).
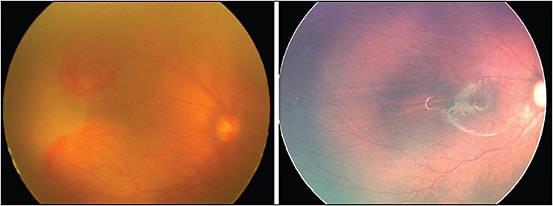
Figure 3. Aggressive posterior ROP at week 35 of gestational age; patient received intravitreal bevacizumab. At week 65 of GA, continued vascularization of the retina without laser.
Further studies have been published in recent years that have continued to demonstrate the efficacy of bevacizumab. Hwang et al studied 54 eyes with type 1 ROP and concluded that bevacizumab and panretinal photocoagulation were both effective treatments in terms of recurrence and complication rates.17 Isaac et al further demonstrated good structural outcomes in both the laser and injection arms in 23 study eyes with type 1 ROP.18
A recent study by Harder et al suggested that 0.375 mg of bevacizumab may be equally effective to the standard 0.625-mg dose. Even smaller, ultralow doses of intravitreal anti-VEGF agents may be effective as well.19
INTRAVITREAL RANIBIZUMAB THERAPY
Bevacizumab was the first anti-VEGF agent to be used and studied in the treatment of ROP, but ranibizumab has been included in an increasing number of studies in recent years. Menke et al studied six eyes with stage 3 ROP with plus disease that were treated with intravitreal ranibizumab. They found that treatment was successful in all cases and suggested that further studies be conducted to evaluate the safety and sequelae of this treatment modality.20
A similar study by Arámbulo et al found that 75% of eyes treated with ranibizumab achieved regression and favorable outcomes,21 concurring with the previous study that ranibizumab is an effective treatment.
A Turkish study of 36 eyes was later published by Erol et al that compared treatment with bevacizumab and ranibizumab, and the authors found that visual outcomes with the two treatments were equivalent.22
CHALLENGES OF INTRAVITREAL ANTI-VEGF AGENTS
While anti-VEGF therapies have proven treatment effects, questions regarding their use persist. As noted above, the BEAT-ROP study was not powered appropriately to address safety. In total, there were seven deaths in the BEAT-ROP trial: five occurred in the bevacizumab group, although this finding was not significant.1 Adverse outcomes, including choroidal rupture, membrane contraction with retinal detachment, and delayed-onset retinal detachment, have also been described following anti-VEGF treatments.23,24
Additional concerns have been raised regarding potential systemic effects of intravitreal anti-VEGF agents, including potential interference with neurodevelopment. In 2012 Sato et al reported detectable systemic levels of bevacizumab.25
A recent study by Lien and colleagues attempted to address concerns regarding neurodevelopment by retrospectively reviewing ROP type I patients who received laser, bevacizumab, or both. Among 61 patients, there was no difference in the Bayley neurodevelopment scale in those patients who received laser vs those receiving intravitreal bevacizumab alone.
However, there were psychomotor and mental impairments found in the infants who received both treatments, either laser first followed by bevacizumab or vice versa.26 The authors hypothesized that these findings may have occurred because the infants had to undergo more procedures and anesthesia, compared to the monotherapy groups.
Also, these patients were treated at a younger age with more type I retinopathy. Continued extensive evaluations of infants are warranted to determine the possible adverse effects after intravitreal anti-VEGF treatments.
In addition to potential side effects, another challenge is the matter of disease recurrence. BEAT-ROP demonstrated a difference between time to recurrence of neovascularization in the two treatment arms. Stage 3+ ROP recurred at up to seven months after intravitreal anti-VEGF compared to laser, which either failed or succeeded by nine weeks. Consequently, these children must be followed closely for an extended period of up to 80 weeks or beyond.27 This requirement poses a challenge when patients are lost to follow-up.
Furthermore, comparing anti-VEGF agents, Erol et al found that the rate of recurrence with ranibizumab might be higher than that with bevacizumab.22 Again, continued, extensive evaluation is needed in the use of intravitreal anti-VEGF agents.
FUTURE OF ROP TREATMENT
The armamentarium for ROP treatment is growing. There are a number of clinical trials currently in progress that seek to increase the body of knowledge for treating ROP. There are currently five ongoing clinical trials assessing the safety and efficacy of anti-VEGF therapy.
Specific areas of current study include the effective doses of both bevacizumab and ranibizumab to determine the smallest dose that effectively treats ROP while minimizing the adverse effects. Alternatives to anti-VEGF therapy for ROP are also under investigation, with an additional seven studies in progress.
While it is not the magic bullet, anti-VEGF is a treatment that can be embraced cautiously.
CONCLUSION
Intravitreal anti-VEGF treatment of ROP is slowly becoming an adopted treatment option across the United States and even more so in resource-poor areas of the world. Advantages include the relative ease of administration compared to laser, allowance of vascularization of the retina, and much less myopia compared with ablative therapy.
In reality, a combination treatment that involves laser and injections could be the ideal paradigm for ROP in the future. More cautious investigation is needed to understand the long-term side effects. The future looks promising, and thanks to continued research, ROP is a more manageable disease. RP
REFERENCES
1. Mintz-Hittner HA, Kennedy KA, Chuang AZ. BEATROP Cooperative Group: Efficacy of intravitreal bevacizumab for stage 3+ retinopathy of prematurity. N Engl J Med. 2011;364:603-615.
2. Chen J, Smith LEH. Retinopathy of prematurity. Angiogenesis. 2007;10:133-140.
3. Painter SL, Wilkinson AR, Desai P, et al. Incidence and treatment of retinopathy of prematurity in England between 1990 and 2011: database study. Br J Ophthalmol. 2015;99:807-811.
4. Darlow BA, Ells AL, Gilbert CE, Gole GA, Quinn GE. Are we there yet? Bevacizumab therapy for retinopathy of prematurity. Arch Dis Child Fetal Neonatal Ed. 2013;98:F170-F174.
5. Smith LEH. Pathogenesis of retinopathy of prematurity. Semin Neonatol. 2003;8:469-473.
6. Hartnett ME. Vascular endothelial growth factor antagonist therapy for retinopathy of prematurity. Clin Perinatol. 2014;41:925-943.
7. Mintz-Hittner HA, Best LM. Antivascular endothelial growth factor for retinopathy of prematurity. Curr Opin Pediatr. 2009;21:182-187.
8. Multicenter trial of cryotherapy for retinopathy of prematurity. Preliminary results. Cryotherapy for Retinopathy of Prematurity Cooperative Group. Arch Ophthalmol. 1988;106:471-479.
9. Early Treatment for Retinopathy Of Prematurity Cooperative Group. Revised indications for the treatment of retinopathy of prematurity: results of the early treatment for retinopathy of prematurity randomized trial. Arch Ophthalmol. 2003;121:1684-1696.
10. Geloneck MM, Chuang, AZ, Mintz-Hittner HA et al. Refractive outcomes following bevacizumab monotherapy compared with conventional laser treatment. JAMA Ophthalmol. 2014;132:1327-1333.
11. Gadkari SS, Kulkarni SR, Kamdar RR, Deshpande M. Successful surgical management of retinopathy of prematurity showing rapid progression despite extensive retinal photocoagulation. Middle East Afr J Ophthalmol. 2015;22:393-395.
12. Gunn DJ, Cartwright DW, Gole GA. Prevalence and outcomes of laser treatment of aggressive posterior retinopathy of prematurity. Clin Exp Ophthalmol. 2014;42:459-465.
13. Klufas MA, Chan RV. Intravitreal anti-VEGF therapy as a treatment for retinopathy of prematurity: what we know after 7 years. J Pediatr Ophthalmol Strabismus. 2015;52:77-84.
14. Micieli JA, Surkont M, Smith AF. A systematic analysis of the offlabel use of bevacizumab for severe retinopathy of prematurity. Am J Ophthalmol. 2009;148:536-543.
15. Lalwani GA, Berrocal AM, Murray TG, et al. Offlabel use of intravitreal bevacizumab (Avastin) for salvage treatment in progressive threshold retinopathy of prematurity. Retina. 2008;28:S13-S18.
16. Law JC, Recchia FM, Morrison DG, Donahue SP, Estes RL. Intravitreal bevacizumab as adjunctive treatment for retinopathy of prematurity. J AAPOS. 2010;14:6-10.
17. Hwang CK, Hubbard GB, Hutchinson AK, Lambert SR. Outcomes after intravitreal bevacizumab versus laser photocoagulation for retinopathy of prematurity: A 5-year retrospective analysis. Ophthalmology. 2015;122:1008-1015.
18. Isaac M, Mireskandari K, Tehrani N. Treatment of type 1 retinopathy of prematurity with bevacizumab versus laser. J AAPOS. 2015;19:140-144.
19. Harder BC, Von Baltz S, Jonas JB, Schlichtenbrede FC. Intravitreal low-dosage bevacizumab for retinopathy of prematurity. Acta Ophthalmol. 2014;92:577-581.
20. Menke MN, Framme C, Nelle M, Berger MR, Sturm V, Wolf S. Intravitreal ranibizumab monotherapy to treat retinopathy of prematurity zone II, stage 3 with plus disease. BMC Ophthalmol. 2015;15:20.
21. Arámbulo O, Dib G, Iturralde J, Duran F, Brito M, Fortes Filho JB. Intravitreal ranibizumab as a primary or a combined treatment for severe retinopathy of prematurity. Clin Ophthalmol. 2015;9:2027-2032.
22. Erol MK, Coban DT, Sari ES, et al. Comparison of intravitreal ranibizumab and bevacizumab treatment for retinopathy of prematurity. Arq Bras Oftalmol. 2015;78:340-343.
23. Azad R. Use of intravitreal antiVEGF: Retinopathy of prematurity surgeons’ in Hamlet’s dilemma? Indian J Ophthalmol. 2011;59;421-422.
24. Jang SY, Choi KS, Lee SJ. Delayed-onset retinal detachment after an intravitreal injection of ranibizumab for zone 1 plus retinopathy of prematurity. J AAPOS. 2010;14:457-458.
25. Sato T, Wada K, Arahori H, et al. Serum concentrations of bevacizumab (avastin) and vascular endothelial growth factor in infants with retinopathy of prematurity. Am J Ophthalmol. 2012;153:327-333.
26. Lien R, Yu M, Hsu K, et al. Neurodevelopmental outcomes in infants with retinopathy of prematurity and bevacizumab treatment. PLoS ONE 2016;11:e0148019.
27. Moshfeghi DM, Berrocal AM. Retinopathy of prematurity in the time of bevacizumab: incorporating the BEAT-ROP results into clinical practice. Ophthalmology. 2011;118:1227-1228.