







An Update on Intraoperative OCT
DISCOVER builds on the results of PIONEER.
PAULA PECEN, MD
Optical coherence tomography was introduced in 1991 as a noninvasive method for imaging nontransparent tissues,1 and it has transformed the field of ophthalmology and significantly affected the diagnosis and management of several retinal diseases. OCT has even driven treatment decisions in clinical trials related to treatment of neovascular age-related macular degeneration,2 retinal vein occlusion,3 and diabetic macular edema.4
While OCT has dominated our clinical decision-making, OCT has only recently been incorporated into our operative surgical decision-making by supplementing our surgical assessments in the operating room as intraoperative OCT (iOCT).
Intraoperative OCT (Figure 1) has previously been described in several types of retina surgery, including vitrectomy with macular hole (Figure 2, page 42), epiretinal membranes (Figure 3, page 44), vitreomacular traction, subretinal tissue plasminogen injection for submacular hemorrhage, and rhegmatogenous retinal detachments.5-11
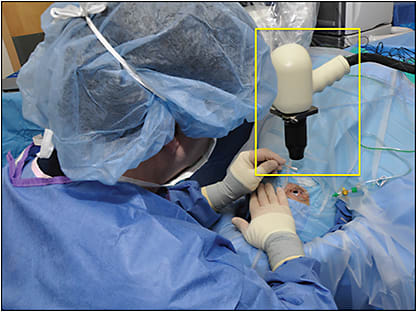
Figure 1. Microscope-mounted portable iOCT system (yellow box).
ALL IMAGES COURTESY OF JUSTIS EHLERS, MD
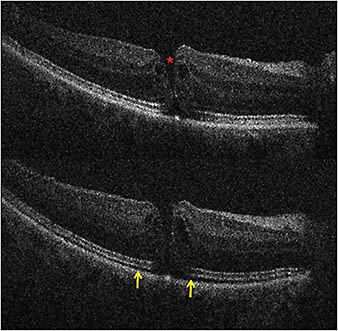
Figure 2. Top) Preincision iOCT B-scan revealing full-thickness macular hole (red asterisk). Bottom) Postpeel iOCT B-scan revealing expansion of the subretinal hyporeflectivity band between the photoreceptor layers and the retinal pigment epithelium (yellow arrows).
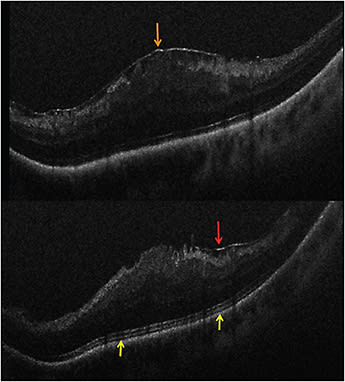
Figure 3. Intraoperative OCT and ERM. (Top) Preincision iOCT B-scan revealing prominent ERM (orange arrow). (Bottom) Postpeel iOCT B-scan revealing expansion of the subretinal hyporeflectivity band between the photoreceptor layers and the RPE (yellow arrows). A residual membrane is also identified (red arrow).
PIONEER STUDY
The Prospective Intraoperative and Perioperative Ophthalmic ImagiNg with Optical CoherEncE TomogRaphy (PIONEER) study was previously conducted at the Cole Eye Institute with two-year results published in 201412; it was an exploratory study to investigate the clinical feasibility, impact on surgeon decision-making, and potential safety of a microscope-mounted portable iOCT system.
Paula Pecen, MD, is a vitreoretinal surgery fellow at the Cole Eye Institute of the Cleveland Clinic in Ohio. She reports no financial interests in any products mentioned in this article. Dr. Pecen can be reached via e-mail at paulaepecen@gmail.com.
The PIONEER study enrolled 531 eyes (275 anterior-segment cases and 256 posterior-segment cases), with iOCT imaging obtained in 98% of eyes. The most common anterior-segment procedure was Descemet stripping automated endothelial keratoplasty (n=135), and the most common posterior-segment procedure was vitrectomy with membrane peeling (n=154).
Surgeon feedback showed that iOCT informed surgeon decision-making in 48% of lamellar keratoplasty cases and 43% of ERM peeling surgeries. The median time to pause surgery and to perform iOCT was 4.9 minutes per scan session, and no adverse events were attributed to iOCT, thus demonstrating the safety, feasibility, and surgical utility of an iOCT system.
DISCOVER STUDY
The follow-up study to the PIONEER study, the Determination of Feasibility of Intraoperative Spectral Domain Microscope Combined/Integrated OCT Visualization During En Face Retinal and Ophthalmic Surgery (DISCOVER) study was also conducted at Cole Eye Institute, with results published in 2015.13
The DISCOVER study was conducted to evaluate a microscope-integrated iOCT system with a heads-up display in one particular iOCT system, the Rescan 700 (Carl Zeiss Meditec, Dublin, CA), which uses the Lumera 7000 (Carl Zeiss Meditec) platform with the standard microscope viewing system for anterior-segment surgery and the Resight lens system or a contact lens system for posterior-segment surgery with iOCT visualization.
During the DISCOVER study, the surgeons could select scan length, angle, and location either via foot-pedal control or input through the video monitor display system with assistance. Most other iOCT systems incorporate the addition of the OCT component to the intraoperative microscope as an add-on system.
This add-on is mounted within the optical path or accessed via a side port to introduce the OCT beam with an OCT engine that resides outside of the surgical microscope, thus altering the overall surgical viewing of the microscope, as well as increasing the size and shape of the microscope within the surgical field.8,14
Earlier iterations of iOCT included handheld imaging and externally mounted systems that required the surgeon to halt surgery to obtain imaging, leading to significant delays in surgery. This stands in contrast to the Rescan 700 iOCT microscope, which has incorporated the OCT technology within the microscope system to minimally alter the overall footprint of the microscope system in the operating room.
The Rescan 700 is one of two commercially available iOCT prototype systems with a heads-up display capability to display real-time iOCT in one of the oculars; the other commercially available system is the Haag-Streit iOCT system (Haag-Streit, Mason, OH). Other heads-up display iOCT microscope prototypes are also currently being developed at Cole and at the Duke Eye Center.15
Initial Results
Initial results from the DISCOVER study published in the British Journal of Ophthalmology in 2014 showed the utilization of the first 10 cases using iOCT in both anterior- and posterior-segment surgery.16 Posterior-segment iOCT imaging included visualization of hyaloid release with triamcinolone acetonide and completeness of peeling in macular hole, ERM, and VMT cases.
One case involving VMT revealed the formation of an occult full-thickness macular hole identified on iOCT after hyaloid elevation, resulting in a change in the surgical procedure, thus performing an internal limiting membrane peel with gas tamponade, instead of a simple fluid-air exchange.
The one-year results of the DISCOVER study published in JAMA Ophthalmology in 2015 included 227 eyes that underwent iOCT imaging with the Rescan 700 system during 91 anterior-segment and 136 posterior-segment surgeries. Successful imaging (defined as the ability to acquire an OCT image of the tissue of interest) was obtained in 224 of 227 eyes (99%).
During lamellar keratoplasty, iOCT data altered surgical decision-making in 38% of cases (eg, iOCT visualization of complete graft apposition when the surgeon initially believed interface fluid was still present).
During vitrectomy with membrane peeling, iOCT data conflicted with the surgeon’s impression of membrane peel completeness in 19% of cases (eg, iOCT displayed a persistent occult residual membrane or showed lack of residual membrane).
For posterior-segment surgery, surgeons reported that use of iOCT provided valuable feedback in 71% (97 of 136) of cases.14 Although use of iOCT created absolute shadowing with real-time membrane peeling using metallic instruments, iOCT was still useful in visualizing tissue-instrument interactions, revealing residual membranes, and confirming completion of surgical objections in macular surgery.
Notably, iOCT was particularly helpful in cases of myopic foveal schisis and vitreoschisis with multilaminar membranes. In retinal detachment surgery, iOCT allowed for the imaging of the retina-retinal pigment epithelium apposition after perfluoro-n-octane (PFO) tamponade and recurrence of subfoveal fluid after air-fluid exchange.
It revealed that, in one case with proliferative vitreoretinopathy, a subretinal band was entirely flat under PFO, leading to abortion of additional membrane peeling, which ultimately minimized surgical manipulation, potentially limiting increased release of RPE cells.
In patients with proliferative diabetic retinopathy, iOCT helped visualize tissue planes to assist surgeon discrimination of retinal tissue and fibrovascular tissue. In choroidal biopsy, the optimal depth for the tissue sample procurement could be imaged with iOCT as well.
REMOVAL OF SUBFOVEAL PFO USING IOCT
One interesting case highlighted a new surgical technique within the DISCOVER study using real-time iOCT feedback to guide surgical maneuvers and to help facilitate surgical removal of chronic subretinal PFO.17
PFO is a widely utilized synthetic compound with a high specific gravity used to flatten detached retina in retinal detachment surgery. A major complication with PFO is retained subretinal PFO requiring surgical evacuation, mainly when a patient is symptomatic with an absolute scotoma and when the PFO has localized to the subfoveal area.
In this particular case, a patient with a prior giant retinal tear and retinal detachment previously underwent surgical repair with a scleral buckle, vitrectomy, PFO, endolaser, and octafluoropropane gas tamponade, with postoperative retained subfoveal PFO and the formation of PVR and inferior redetachment.
Three months after the retinal detachment surgery, the patient elected to undergo surgical repair and was enrolled in the DISCOVER study. A 41-gauge needle was used to create a subretinal bleb in the superotemporal fovea in an attempt to displace the subfoveal PFO; however, iOCT showed the presence of either very adherent or loculated PFO within the retinal tissue that did not displace the PFO within the subretinal bleb.
Preretinal PFO was then instilled, again without the displacement of the subfoveal PFO, confirming the loculated nature of the subretinal PFO. Although the patient had inferior membranes and subretinal fluid, the inferior retina was too atrophic to reflect for removal of the subfoveal PFO directly.
Thus, iOCT guided a parafoveal entry of a 41-gauge needle to successfully aspirate the PFO. Then, the peripheral retinal detachment was repaired. In addition to confirming the anatomic location of the PFO, iOCT was key to guiding the ultimate successful PFO removal due to decreasing surgical visualization related to worsening corneal edema.
FUTURE DIRECTIONS
Microscope integration of OCT with heads-up display can provide real-time visualization of tissue-instrument interaction, as well as rapid localization of pathology and anatomy that may not otherwise be apparent during surgery. Thus, it can provide significant and measurable surgical advantages.
These advances will likely attract more extensive utilization of iOCT as an assistive device in ophthalmic surgery. Further advances in surgical instrumentation to improve real-time visualization intraoperatively will help to advance the use of iOCT by developing materials that minimize scatter yet allow for transmission of light from OCT.18
Furthermore, automated iOCT tracking to areas of interest will need to be developed to minimize the surgeon burden of manually aiming iOCT scans while operating. Improved software analysis programs may also help analyze various retinal pathologies, eg, macular hole morphology, and might potentially improve surgeon understanding of macular hole closure to individualize patient care, based on certain findings on macular hole shape or size at the end of a macular hole surgery.
Although iOCT is still currently more of a research tool, further refining its ability to improve surgical decision-making and possibly impact surgical outcomes, while improving efficiency and ease of use intraoperatively, will ultimately drive this tool into mainstream use. RP
REFERENCES
1. Huang D, Swanson EA, Lin CP, et al. Optical coherence tomography. Science. 1991;254:1178-1181.
2. Comparison of Age-related Macular Degeneration Treatment Trials (CATT) Research Group; Martin DF, Maguire MG, Fine SL, et al. Ranibizumab and bevacizumab for treatment of neovascular age-related macular degeneration: two-year results. Ophthalmology. 2012;119:1388-1398.
3. Heier JS, Clark WL, Boyer DS, et al. Intravitreal aflibercept injection for macular edema due to central retinal vein occlusion: two-year results from the COPERNICUS study. Ophthalmology. 2014;121:1414-1420.
4. Wells JA, Glassman AR, Ayala AR, et al. Aflibercept, bevacizumab, or ranibizumab for diabetic macular edema: two-year results from a comparative effective randomized clinical trial. Ophthalmology. 2016 Feb 27. [Epub ahead of print]
5. Dayani PN, Maldonado R, Farsiu S, Toth CA. Intraoperative use of handheld spectral domain optical coherence tomography imaging in macular surgery. Retina. 2009;29:1457-1468.
6. Ray R, Baranano DE, Fortun JA, et al. Intraoperative microscope-mounted spectral domain optical coherence tomography for evaluation of retinal anatomy during macular surgery. Ophthalmology. 2011;118:2212-2217.
7. Binder S, Falkner-Radler CI, Hauger C, et al. Feasibility of intrasurgical spectral-domain optical coherence tomography. Retina. 2011;31:1332-1336.
8. Ehlers JP, Ohr MP, Kaiser PK, Srivastava SK. Novel microarchitectural dynamics in rhegmatogenous retinal detachments identified with intraoperative optical coherence tomography. Retina. 2013;33:1428-1434.
9. Ehlers JP, Tam T, Kaiser PK, et al. Utility of intraoperative optical coherence tomography during vitrectomy surgery for vitreomacular traction syndrome. Retina. 2014;34:1341-1346.
10. Ehlers JP, Xu D, Kaiser PK, et al. Intrasurgical dynamics of macular hole surgery: an assessment of surgery-induced ultrastructural alterations with intraoperative optical coherence tomography. Retina. 2014;34:213-221.
11. Ehlers JP, Petkovsek DS, Yuan A, Singh RP, Srivastava SK. Intrasurgical assessment of subretinal tPA injection for submacular hemorrhage in the PIONEER study utilizing intraoperative OCT. Ophthalmic Surg Lasers Imaging Retina. 2015;46:327-332.
12. Ehlers JP, Dupps WJ, Kaiser PK, et al. The prospective intraoperative and perioperative ophthalmic imaging with optical coherence tomography (PIONEER) study: 2-year results. Am J Ophthalmol. 2014;158:999-1007.
13. Ehlers JP, Goshe J, Dupps WJ, et al. Determination of feasibility and utility of microscope-integrated optical coherence tomography during ophthalmic surgery: the DISCOVER study RESCAN results. JAMA Ophthalmol. 2015;133:1124-1132.
14. Ehlers JP, Tao YK, Farsiu S, et al. Integration of a spectral domain optical coherence tomography system into a surgical microscope for intraoperative imaging. Invest Ophthalmol Vis Sci. 2011;52:3153-3159.
15. Ehlers JP, Tao YK, Srivastava SK. The value of intraoperative optical coherence tomography imaging in vitreoretinal surgery. Curr Opin Ophthalmol. 2014;25:221-227.
16. Ehlers JP, Kaiser PK, Srivastava SK. Intraoperative optical coherence tomography using the RESCAN 700: preliminary results from the DISCOVER study. Br J Ophthalmol. 2014;98:1329-1332.
17. Smith AG, Cost BM, Ehlers JP. Intraoperative OCT-assisted subretinal perfluorocarbone liquid removal in the DISCOVER study. Ophthalmic Surg Lasers Imaging Retina. 2015;46:964-966.
18. Ehlers JP, Srivastava SK, Feiler D, et al. Integrative advances for OCT-guided ophthalmic surgery and intraoperative OCT: microscope integration, surgical instrumentation, and heads-up display surgeon feedback. PLoS One. 2014;9:e105224.