







CODING Q&A
Microperimetry Utility and Reimbursement
SUZANNE L. CORCORAN, COE
With retinal pathology, the treating physician observes both structure and function to evaluate and manage conditions such as age-related macular degeneration. Imaging, including photography, angiography, and tomography, identifies the structural changes, while psychophysical tests, including visual acuity, color vision, contrast sensitivity, and perimetry, identify changes in function. Fundus perimetry, better known as microperimetry, allows precise correlation of structure and function, in real time, by superimposing the retinal sensitivity threshold, on a point-by-point basis, over an image produced with scanning laser ophthalmoscopy (Figure, page 16). Microperimetry also quantifies fixation characteristics by defining the preferred retinal locus fixation site in relation to scotoma. Significantly, follow-up examinations using microperimetry allow for re-evaluation of exactly the same retinal points. This has clinical value for assessing treatment outcomes and disease progression. Compared to standard perimetry, microperimetry offers several advantages, particularly for patients who have great difficulty maintaining fixation.
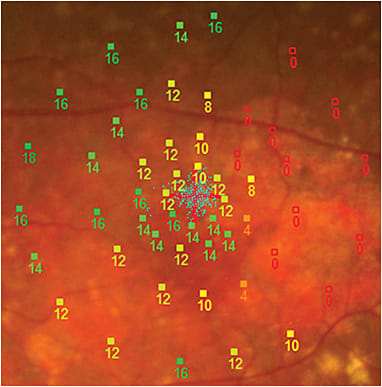
Figure. Microperimetry
Suzanne L. Corcoran, COE, is executive vice president and founder of Corcoran Consulting Group, San Bernardino, CA, which specializes in coding and reimbursement issues for ophthalmic practices. Her e-mail is scorcoran@corcoranccg.com.
MICROPERIMETRY FEATURES
Instrumentation that incorporates microperimetry is very flexible and offers the user a number of choices:
• Variable light stimuli (luminance)
• Variable stimulus size (Goldmann I to V)
• Variable fixation target size and shape
• Variable presentation time
• Static or kinetic testing protocol
• Variable threshold strategies, 4-2-1 staircase, 4-2 staircase, and fast strategy
• Mesopic testing with or without dilation
• Variable test grid, position, and number of spots
• Fully automatic, semiautomatic, or manual operation.
Test results are reported in decibels (dB) or pseudocolor maps on top of the fundus photograph or infrared (IR) image. Testing requires five to six minutes for 45 stimuli, and seven to nine minutes for 77 stimuli in a healthy subject, but longer when pathology is present.
Coincident with microperimetry, a fixation exam identifies fixation positions, typically within 60 seconds.1
CODING AND REIMBURSEMENT
Classic visual field examinations are distinguished within the AMA’s Current Procedural Terminology (CPT) handbook by the extent of the test. They include:
• 92081 – limited exam, single stimulus
• 92082 – intermediate exam, suprathreshold
• 92083 – extended exam, threshold
Microperimetry, whose nearest standard perimetry counterpart is Humphrey 10-2, is properly categorized as a threshold test – CPT 92083. The fixation exam is an incidental part of the visual field exam, and not separately reportable. The concurrent fundus photograph or other image is separately reportable, and the National Correct Coding Initiative does not bundle perimetry with imaging — both are reimbursed on the same day.
While reimbursement for visual field testing is most commonly associated with glaucoma, coverage policies of most payers, including Medicare, also include a number of other covered indications within the category of retinal disease (361.xx, 362.xx, 363.xx).
Medicare’s National Coverage Determination (NCD) §80.9 – Computer Enhanced Perimetry states, “Computer enhanced perimetry involves the use of a micro-computer to measure visual sensitivity at pre-selected locations in the visual field. It is a covered service when used in assessing visual fields in patients with glaucoma or other neuropathologic defects.”
By way of amplification, the introduction to the NCD states, “Where coverage of an item or service is provided for specified indications or circumstances but is not explicitly excluded for others, or where the item or service is not mentioned at all in the CMS Manual System, the Medicare contractor is to make the coverage decision, in consultation with its medical staff, and with CMS when appropriate, based on the law, regulations, rulings and general program instructions.” Consequently, it is necessary to check your local Medicare policy for additional information regarding covered indications and diagnoses beyond the NCD.
DOCUMENTATION
For perimetry, CPT’s description includes the phrase “with interpretation and report.” A reader might ask, with good reason, what exactly is meant by this phrase; further, what kind of chart note is required? Because diagnostic tests accompany almost every eye exam ophthalmologists perform on Medicare beneficiaries, this question takes on added urgency, given that insufficient chart documentation is reason enough to require repayment of any reimbursement.
The Medicare guidelines for interpretation of diagnostic tests are discussed in Medicare Claims Process Manual (MCPM) Chapter 13 §100 Interpretation of Diagnostic Tests. CMS makes a distinction between a review of a test and an “interpretation and report”.
“Carriers generally distinguish between an ‘interpretation and report’ of an x-ray or an EKG procedure and a ‘review’ of the procedure. A professional component billing based on a review of the findings of these procedures, without a complete, written report similar to that which would be prepared by a specialist in the field, does not meet the conditions for separate payment of the service. This is because the review is already included in the … E/M payment,” it reads.
The review of a test is not separately payable because it is part of an evaluation and management (E/M) service.
“For example, a notation in the medical records saying ‘fx-tibia’ or ‘EKG-normal’ would not suffice as a separately payable interpretation and report of the procedure and should be considered a review of the findings payable through the E/M code. An ‘interpretation and report’ should address the findings, relevant clinical issues, and comparative data (when available).”
Simple, brief notations such as “normal” or “abnormal” are construed as a review of the test rather than as an interpretation and report. As a condition of payment, 42 CFR 415.120 (a) states:
“(a) Services to beneficiaries. The carrier pays for radiology services furnished by a physician to a beneficiary on a fee schedule basis only if the services meet the conditions for fee schedule payment in §415.102(a) and are identifiable, direct, and discrete diagnostic or therapeutic services furnished to an individual beneficiary, such as interpretation of x-ray plates, angiograms, myelograms, pyelograms, or ultrasound procedures. The carrier pays for interpretations only if there is a written report prepared for inclusion in the patient’s medical record maintained by the hospital.”
The value of an interpretation and report derives from the answers to important questions about the diagnostic test. These include:
• Physician’s order – Why is the test desired?
• Date performed – When was it performed?
• Technician’s initials – Who did it?
• Reliability of the test – Was the test of any value?
• Patient cooperation – Was the patient at fault?
• Test findings – What are the results of the test?
• Assessment, diagnosis – What do the results mean?
• Impact on treatment, prognosis – What’s next?
• Physician’s signature – Who is the physician?
Tests, such as perimetry, are much more valuable for making decisions about treatment when a series exists. Then, the concept of comparative data cited above is particularly meaningful. Does the series demonstrate disease progression?
For microperimetry, the interpretation and report might read something like this:
• August 27, 2014
• Technician: Mae West, COA
• Excellent reliability
• Good patient cooperation
• Findings: Neovascular AMD, OU. Central, unstable fixation. Dense central scotomas, OD>OS.
• Dx: Neovascular AMD, shows progression OD since last microperimetry (Jan 2014)
• Plan: Retreat OD with anti-VEGF intravitreal injection
• Signed: I. C. Better, MD
Following a test, your interpretation and report do not need to be book length, but they must answer pertinent questions about the service. A cryptic, one-word note isn’t an interpretation as Medicare understands that term.
CONCLUSION
Microperimetry is a valuable diagnostic tool for assessing common and uncommon retinal diseases. It integrates information about structural and functional changes so the ophthalmologist can better evaluate and treat these conditions. Additionally, microperimetry has applications for the low-vision specialist who must identify the remaining parts of the macula that provide some vision and teach the patient to use them.
From a reimbursement perspective, both the imaging and perimetry are separately reimbursed for covered indications even though they occur at the same time. Microperimetry testing uses a threshold protocol so CPT 92083 applies. Chart notes for the interpretation and report must not be abbreviated, such as using a single word. Instead, a complete and informative chart note is required for proper reimbursement. RP