







Advances in the Treatment of Retinoblastoma
The most recent data suggest that combination treatments are obtaining greater efficacy.
VICTOR M. VILLEGAS, MD • AARON S. GOLD, OD • ANDREA WILDNER, CRA • DITTE J. HESS, CRA • FIONA J. EHLIES, BSC, CDOS • THEODORE J. LAMPIDIS, PhD • TIMOTHY G. MURRAY, MD, MBA
The management of retinoblastoma (RB) continues to change as new strategies focus on local treatments. Extensive research developments have significantly altered the management of RB, providing new hope to patients.
Management of RB tumors requires a multidisciplinary approach that may include an ocular oncologist, pediatric oncologist, pediatric ophthalmologist, pediatrician, interventional radiologist, and ocular pathologist.
Individualized treatment, considering factors such as the International Classification (IC) of RB, laterality, location of tumors, patient age, family history, and prior treatment, must be considered.1-2
Retinoblastoma treatment aims at child survival. Globe salvage and preservation of vision are secondary goals. Early diagnosis remains the most crucial step in decreasing morbidity and mortality.3
CURRENT STANDARDS OF CARE
Small tumors (≤3 mm) may be amenable to thermotherapy.4 Laser treatments may be repeated monthly until complete tumor regression is documented. Indirect fundoscopy may determine tumor regression or inactivity.5 Intravenous chemotherapy may be effective in advanced tumors that are not amenable to ablation treatment.
Victor M. Villegas, MD, Aaron S. Gold, OD, Andrea Wildner, CRA, and Fiona J. Ehlies, BSc, CDOS, are with Murray Ocular Oncology and Retina in Miami, FL. Ditte J. Hess, CRA, is with Bascom Palmer Eye Institute in Miami. Theodore J. Lampidis, PhD, is on faculty of the Department of Cell Biology and Anatomy at the University of Miami Miller School of Medicine. Timothy G. Murray, MD, MBA, is a partner at Murray Ocular Oncology and Retina. None of the authors reports any financial interests in products mentioned in this article. Dr. Murray’s e-mail is TMurray@med.miami.edu.
The classic three-drug systemic treatment (carboplatin [Paraplatin, Bristol-Myers Squibb, New York, NY], vincristine, and etoposide) is not without risks. Bone marrow suppression, ototoxicity, nephrotoxicity, and risk of induction of secondary cancers have been reported.6-7
Patients typically undergo multiple treatments, and hereditary cases routinely undergo chemoreduction to prevent intracranial neuroblastic malignancies.8-9 Combined treatment has been more efficacious for tumor control than chemoreduction alone in both small and large tumors.10-13
A recent study by Murray and associates demonstrated that chemoreduction with aggressive local consolidation of both foveal and extrafoveal tumors achieved tumor control in 83% of R-E Group V tumors.14 All tumors less than R-E Group V status achieved 100% control. Despite ablative foveal laser treatment, 56% of eyes had better than 20/80 visual acuity.
Enucleation remains the standard treatment for Group E RB.15 Histopathologic analysis can determine whether adjuvant treatment is necessary, depending on high-risk criteria.16 Adjuvant therapy postenucleation decreased metastasis in advanced RB from 24% of children to 4% when treated with adjuvant chemotherapy.17
SUPERSELECTIVE INTRA-ARTERIAL CHEMOTHERAPY
Japanese physicians introduced the technique of ophthalmic arterial infusion therapy for patients with intraocular RB.18 The study technique consisted of selective catheterization of the internal carotid artery, followed by the occlusion of a balloon distal to the ophthalmic artery.
During the temporary occlusion of the internal carotid artery, melphalan (Alkeran, Celgene, Summit, NJ) was infused into the catheter tip and into the ophthalmic artery.
The study treated 187 patients with no reported serious complications. The most common complications were mild, transient bradycardia, periorbital erythema, and swelling. Melphalan could be successfully administered to the ophthalmic artery 97.51% of the time.18
To prevent the need to occlude distal flow with the subsequent risk of ischemic events, more advanced techniques were developed to selectively cannulate the ophthalmic artery.
More Recent Research
In recent studies, Abramson and associates have reported significant tumor control and stabilization of vision in children with R-E Group V tumors without severe side effects.19-20 Only one patient from their studies had disease progression that needed enucleation. No patients received systemic chemotherapy or radiation.
Further studies by the same group reported four patients with bilateral R-E Group V who were initially treated bilaterally.20 All of the patients avoided enucleation or radiation. No significant adverse effects were observed.
Studies performed by Murray and coworkers, evaluating selective ophthalmic artery infusion with melphalan in patients with R-E Group V tumors who failed prior systemic chemotherapy and laser consolidation, showed significant benefits in advanced disease (Figure 1).21
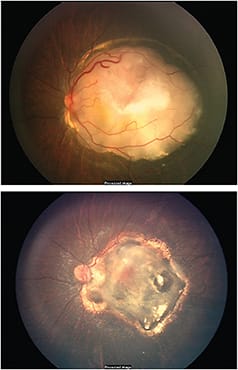
Figure 1. Retinoblastoma before (top) and after (bottom) selective ophthalmic artery infusion with melphalan.
The study evaluated 12 eyes of 10 children. All of the patients underwent selective ophthalmic artery infusion with melphalan without complications. Tumor control was present in 75% of eyes at six months without evidence of progression. Three eyes were enucleated secondary to tumor progression. Neutropenia was reported in four children.
Ocular adverse effects included intraretinal hemorrhages, peripapillary cotton wool spots, vitreous hemorrhages, and myositis. Histopathology of the three enucleated eyes showed high-risk characteristics in two eyes with persistent retinoblastoma tumors in all eyes.22 No anterior-segment or extraocular extension occurred in any of the eyes analyzed.
A recent study also investigated the use of combination therapy via selective ophthalmic artery infusion,23 evaluating 57 carboplatin with or without topotecan (Hycamtin, GlaxoSmithKline, Philadelphia, PA) infusions in 31 eyes of 24 patients. All the patients were alive, and none developed a second malignancy at a median follow-up of 25 months.
Overall ocular survival was 89.9% at two years. Carboplatin therapy had no significant effect on electroretinogram responses at three months or at one year when evaluated by both maximum and cumulative carboplatin doses.
In addition, analysis of electroretinogram responses following infusions containing carboplatin only and carboplatin with topotecan revealed no statistically significant changes.
The Evidence in Summary
These findings suggest that selective intra-arterial combination therapy with topotecan, carboplatin, and/or melphalan is effective in the treatment of RB and decreases the toxic window during treatment, especially in patients that need bilateral therapy.
Cannulation of the ophthalmic artery is difficult in children, particularly in infants younger than age 6 months. Such young infants might benefit from initial intravenous chemotherapy, followed by intra-arterial chemotherapy (Figure 2, page 32).24
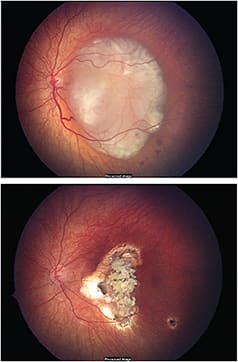
Figure 2. Retinoblastoma before (top) and after (bottom) intra-arterial chemotherapy.
Superselective intra-arterial chemotherapy delivers targeted, high-dose chemotherapy to the eyes of children with RB. Preliminary studies have demonstrated the effectiveness of this novel therapy both as salvage and primary management. No deaths or strokes have been observed, but vision-threatening vascular complications have been reported.
Long-term studies evaluating superselective intra-arterial chemotherapy are needed to determine safety and efficacy in patients with RB. Minimizing systemic adverse events in patients with RB with local chemotherapy may benefit a specific subset of patients. Patients with hereditary RB may benefit the most from systemic chemotherapy, to prevent late-onset intracranial malignancies.
INTRAVITREAL CHEMOTHERAPY
Intravitreal injection therapy for RB has shown promise in the treatment of vitreous seeds.25 The potential for tumor dissemination following intravitreal penetration has limited its use. Many authors have reported on the efficacy of intravitreal melphalan for the treatment of RB.26-28 Intravitreal melphalan was recently investigated for recurrent vitreous seeds following previous therapies of intra-arterial chemotherapy or systemic chemoreduction (Figure 3).29

Figure 3. Vitreous seeds of retinoblastoma following previous chemotherapy.
Eyes treated with low-dose melphalan (8-10 μg) showed less control and minimal side effects, whereas those treated with higher doses (30-50 μg) showed excellent control. The 50-μg dose was toxic, with persistent hypotonia and phthisis bulbi. No extraocular tumor seeding occurred.
A recent Columbia University study evaluated the risk of extraocular tumor spread in 304 patients receiving therapeutic intravitreal injections for RB.30
Only one patient had extraocular tumor spread, as well as one patient in whom intravitreal treatment could not be excluded as a contributor to metastatic disease. The proportion of subjects with extraocular tumor spread potentially due to intravitreal treatment in these combined reports was 0.007 (95% CI 0.0008 to 0.0236), with a mean follow-up of 72.1 months.
In a subset of 61 patients receiving intravitreal treatment via a safety-enhancing injection technique (347 injections, mean 19.6 months of follow-up), no reports emerged of tumor spread. The authors concluded that RB metastasis following intravitreal therapy is rare and should not preclude its clinical use in appropriately selected cases.
Further studies are necessary to assess long-term intravitreal therapy safety and to better delineate its role in the management of retinoblastoma. The adoption of specific guidelines for intravitreal treatment case selection and additional data on potential ocular toxicity remain essential to enabling more widespread use of this treatment.
PERIOCULAR CHEMOTHERAPY
Systemic chemotherapy has been associated with severe systemic toxicities, including the development of secondary malignancies. Multiple delivery mechanisms have been employed to minimize the systemic effects in patients that would not benefit from systemic treatment.
Abramson et al have performed studies using subconjunctival carboplatin in Group C and D eyes; however, the results have been unsatisfactory.31 Additionally, Leng and colleagues showed that focal subconjunctival carboplatin chemotherapy controlled unilateral early progressive retinoblastoma.32
Focal subconjunctival injection of carboplatin may potentially be an adjuvant for both small and large tumors. The side effects of periocular carboplatin include strabismus, optic neuropathy, periocular inflammation, and fat atrophy.33-35 Periocular inflammation associated with periocular carboplatin has limited its widespread use in children with RB.
The Most Recent Data
Recent studies have also reported the efficacy of periocular topotecan in patients with RB. Ten eyes from eight patients were enrolled in the study. Patients received one to four injections of periocular topotecan in fibrin sealant, without or with concomitant laser.
Six children with IC Group A and B eyes responded favorably to treatment. Two children with IC Group D eyes were not controlled by periocular topotecan as an adjuvant to systemic chemotherapy. Toxic hematological effects were self-limiting and included decreased hemoglobin, absolute neutrophil, white blood cells, and platelet counts. Prospective studies are necessary to assess the role of local chemotherapies for the treatment of RB.
NEW FRONTIERS
New research has expanded our understanding of the tumorigenesis and the tumor microenvironment.36 Angiogenesis plays a key role in the development of malignant tumors. During tumor growth, VEGF levels increase owing to cellular stress, such as hypoxia, and to changes in the tumor microenvironment.
VEGF plays multiple roles during various steps of tumor progression by stimulating vessel growth to provide the necessary metabolic needs. Growing evidence also exists that the p53 tumor suppressor downregulates VEGF expression.37 The exact mechanism by which p53 interacts with VEGF is still unknown.
Glycolytic Inhibitors
Inhibition of glucose metabolism has recently become an attractive target for cancer treatment. Glycolytic inhibitors, such as 2-deoxy-d-glucose (2-DG), target the cellular mechanism that hypoxic tumoral cells utilize for survival.
Unlike cells in normoxic conditions, the cells in the hypoxic regions must use anaerobic glycolysis as their sole sources of energy. 2-DG competes with glucose for cellular transporters and key glycolytic enzymes.
As a result, 2-DG inhibits the metabolic machinery of tumoral cells. Studies have shown that 2-DG decreases angiogenesis and hypoxia both in vitro and in vivo.38-39
Glycolytic inhibitors have been shown to have a synergistic effect on tumor control when used in combination with chemotherapy. Recent studies have shown that 2-DG not only enhanced tumor control in an animal model of RB, but it also permitted the use of lower, subtherapeutic concentrations of periocular carboplatin to decrease tumor burden.40
Antiangiogenic Agents
Antiangiogenic agents have proved to be effective antitumoral agents. In a recent study, the antiangiogenic agent anecortave acetate (Retaane, Alcon, Fort Worth, TX) significantly controlled tumor burden in a murine model of RB when used as monotherapy or as adjuvant therapy.41
Bevacizumab (Avastin, Genentech, South San Francisco, CA) has also been shown to decrease tumor burden both in vitro and in vivo.42 A study performed by Lee et al induced a 75% reduction in the growth of RB without producing significant systemic toxicity.42
A recent study by Murray et al evaluated the effect of optimally timed combination treatment with angiogenic and glycolytic inhibitors on tumor burden, hypoxia, and angiogenesis in advanced retinoblastoma tumors.43
Combination therapy with angiogenic and glycolytic inhibitors significantly enhanced tumor control. The study showed synergistic effects to be dependent on the temporal course of treatment. This study was the first to demonstrate the combined treatment of advanced retinoblastoma tumors in the LHBETATAG mouse model with angiogenic inhibitors and glycolytic inhibitors, avoiding chemotherapy.
Previous studies have implicated the MDMX protein in the suppression of the p53 pathway in retinoblastoma and shown that the MDM2/MDMX antagonist, nutlin-3a, can efficiently induce p53-mediated cell death in retinoblastoma cell lines.44-47 Brennan et al developed an ocular formulation of periocular nutlin and tested the pharmacokinetics and efficacy of this new formulation in genetic and human retinoblastoma orthotopic xenograft models of retinoblastoma.48
Periocular nutlin, combined with systemic topotecan, significantly reduced RB tumor burden compared to systemic topotecan alone in human orthotopic xenografts.48
CONCLUSION
We anticipate clinical trials on the safety and efficacy of these agents in the treatment of human retinoblastoma. Combination treatments with novel adjuvant agents that target the tumor microenviroment hold promise in the treatment of retinoblastoma.
Further laboratory studies are necessary to identify additional targets for treatment, as well as to determine combined multimodal treatments, such as chemotherapy, angiogenic inhibitors, and glycolytic inhibitors. RP
REFERENCES
1. Shields CL, Shields JA. Basic understanding of current classification and management of retinoblastoma. Curr Opin Ophthalmol. 2006;17:228-234.
2. Shields CL, Shields JA. Retinoblastoma management: advances in enucleation, intravenous chemoreduction, and intra-arterial chemotherapy. Curr Opin Ophthalmol. 2010;21:203-212.
3. Leander C, Fu LC, Pena A, et al. Impact of an education program on late diagnosis of retinoblastoma in Honduras. Pediatr Blood Cancer. 2007;49:817-819.
4. Shields CL, Santos MC, Diniz W, et al. Thermotherapy for retinoblastoma. Arch Ophthalmol. 1999;117:885-893.
5. Schefler AC, Cicciarelli N, Feuer W, Toledano S, Murray TG. Macular retinoblastoma: evaluation of tumor control, local complications, and visual outcomes for eyes treated with chemotherapy and repetitive foveal laser ablation. Ophthalmology. 2007;114:162-169.
6. Jehanne M, Lumbroso-Le Rouic L, Savignoni A, et al. Analysis of ototoxicity in young children receiving carboplatin in the context of conservative management of unilateral or bilateral retinoblastoma. Pediatr Blood Cancer. 2009;52:637-643.
7. Bartuma K, Pal N, Kosek S, Holm S, All-Ericsson C. A 10-year experience of outcome in chemotherapy-treated hereditary retinoblastoma. Acta Ophthalmol. 2013 Oct 7. [Epub ahead of print]
8. De Potter P, Shields CL, Shields JA. Clinical variations of trilateral retinoblasto ma: a report of 13 cases. J Pediatr Ophthalmol Strabismus. 1994;31:26-31.
9. Shields CL, Meadows AT, Shields JA, Carvalho C, Smith AF. Chemoreduction for retinoblastoma may prevent intracranial neuroblastic malignancy (trilateral retinoblastoma). Arch Ophthalmol. 2001;119:1269-1272.
10. Shields CL, Mashayekhi A, Au AK, et al. The International Classification of Retinoblastoma predicts chemoreduction success. Ophthalmology. 2006;113:2276-2280.
11. Rodriguez-Galindo C, Wilson MW, Haik BG, et al. Treatment of intraocular retinoblastoma with vincristine and carboplatin. J Clin Oncol. 2003;21:2019-2025.
12. Gombos DS, Kelly A, Coen PG, Kingston JE, Hungerford JL. Retinoblastoma treated with primary chemotherapy alone: the significance of tumour size, location, and age. Br J Ophthalmol. 2002;86:80-83.
13. Shields CL, Mashayekhi A, Cater J, Shelil A, Meadows AT, Shields JA. Chemoreduction for retinoblastoma: analysis of tumor control and risks for recurrence in 457 tumors. Trans Am Ophthalmol Soc. 2004;102:35-44. discussion 44-35.
14. Schefler AC, Cicciarelli N, Feuer W, Toledano S, Murray TG. Macular retinoblastoma: evaluation of tumor control, local complications, and visual outcomes for eyes treated with chemotherapy and repetitive foveal laser ablation. Ophthalmology. 2007;114:162-169.
15. Honavar SG, Singh AD. Management of advanced retinoblastoma. Ophthalmol Clin North Am. 2005;18:65-73,viii.
16. Eagle RC Jr. High-risk features and tumor differentiation in retinoblastoma: a retrospective histopathologic study. Arch Pathol Lab Med. 2009;133:1203-1209.
17. Honavar SG, Singh AD, Shields CL, et al. Postenucleation adjuvant therapy in high-risk retinoblastoma. Arch Ophthalmol. 2002;120:923-931.
18. Yamane T, Kaneko A, Mohri M. The technique of ophthalmic arterial infusion therapy for patients with intraocular retinoblastoma. Int J Clin Oncol. 2004;9:69-73.
19. Abramson DH, Dunkel IJ, Brodie SE, Kim JW, Gobin YP. A phase I/II study of direct intraarterial (ophthalmic artery) chemotherapy with melphalan for intraocular retinoblastoma initial results. Ophthalmology. 2008;115:1398-1404.e1.
20. Abramson DH, Dunkel IJ, Brodie SE, Marr B, Gobin YP. Superselective ophthalmic artery chemotherapy as primary treatment for retinoblastoma (chemosurgery). Ophthalmology. 2010;117:1623-1629.
21. Mutapcic L, Murray TG, Aziz-Sultan MA, et al. Supraselective intra-arterial chemotherapy: evaluation of treatment related complications in advanced refractory retinoblastoma. Clin Ophthalmol. 2014 in press.
22. Mutapcic L, Murray TG, Aziz-Sultan MA, et al. Clinicopathologic review of enucleated eyes after intra-arterial chemotherapy with melphalan for advanced retinoblastoma. Arch Ophthalmol. 2014 in press.
23. Francis JH, Gobin YP, Dunkel IJ, et al. Carboplatin +/- topotecan ophthalmic artery chemosurgery for intraocular retinoblastoma. PLoS One. 2013;8:e72441.
24. Gobin YP, Dunkel IJ, Marr BP, Francis JH, Brodie SE, Abramson DH. Combined, sequential intravenous and intra-arterial chemotherapy (bridge chemotherapy) for young infants with retinoblastoma. PLoS One. 2012;7:e44322.
25. Villegas VM, Hess DJ, Wildner A, Gold AS, Murray TG. Retinoblastoma. Curr Opin Ophthalmol. 2013;24:581-588.
26. Sun YB, Hui P, Punyara K, Bi MC, Li SH, Teng SY, Song E. Intravitreal injection of melphalan in the treatment of retinoblastoma with vitreous cavity seeding. Chin Med J (Engl). 2013;126:1587.
27. Brodie SE, Munier FL, Francis JH, Marr B, Gobin YP, Abramson DH. Persistence of retinal function after intravitreal melphalan injection for retinoblastoma. Doc Ophthalmol. 2013;126:79-84.
28. Munier FL, Gaillard MC, Balmer A, et al. Intravitreal chemotherapy for vitreous disease in retinoblastoma revisited: from prohibition to conditional indications. Saudi J Ophthalmol. 2013;27:147-150.
29. Ghassemi F, Shields CL. Intravitreal melphalan for refractory or recurrent vitreous seeding from retinoblastoma. Arch Ophthalmol 2012;130:1268-1271.
30. Smith SJ, Smith BD. Evaluating the risk of extraocular tumour spread following intravitreal injection therapy for retinoblastoma: a systematic review. Br J Ophthalmol. 2013;97:1231-1236.
31. Abramson DH, Frank CM, Dunkel IJ. A phase I/II study of subconjunctival carboplatin for intraocular retinoblastoma. Ophthalmology. 1999;106:1947-1950.
32. Leng T, Cebulla CM, Schefler AC, Murray TG. Focal periocular carboplatin chemotherapy avoids systemic chemotherapy for unilateral, progressive retinoblastoma. Retina. 2010;30:S66-S68.
33. Mulvihill A, Budning A, Jay V, et al. Ocular motility changes after subtenon carboplatin chemotherapy for retinoblastoma. Arch Ophthalmol. 2003;121:1120-1124.
34. Schmack I, Hubbard GB, Kang SJ, Aaberg TM Jr, Grossniklaus HE. Ischemic necrosis and atrophy of the optic nerve after periocular carboplatin injection for intraocular retinoblastoma. Am J Ophthalmol. 2006;142:310-315.
35. Mallipatna AC, Dimaras H, Chan HS, Héon E, Gallie BL. Periocular topotecan for intraocular retinoblastoma. Arch Ophthalmol. 201;129:738-745.
36. Houston SK, Lampidis TJ, Murray TG. Models and discovery strategies for new therapies of retinoblastoma. Expert Opin Drug Discov. 2013;8:383-394.
37. Farhang Ghahremani M, Goossens S, Nittner D, et al. p53 promotes VEGF expression and angiogenesis in the absence of an intact p21-Rb pathway. Cell Death Differ. 2013;20:888-897.
38. Piña Y, Decatur C, Murray TG, et al. Retinoblastoma treatment: utilization of the glycolytic inhibitor, 2-deoxy-2-fluoro-D-glucose (2-FG), to target the chemoresistant hypoxic regions in LH(BETA)T(AG) retinal tumors. Invest Ophthalmol Vis Sci. 2012;53:996-1002.
39. Piña Y, Houston SK, Murray TG, et al. Retinoblastoma treatment: impact of the glycolytic inhibitor 2-deoxy-d-glucose on molecular genomics expression in LH(BETA)T(AG) retinal tumors. Clin Ophthalmol. 2012;6:817-830.
40. Boutrid H, Jockovich ME, Murray TG, et al. Targeting hypoxia, a novel treatment for advanced retinoblastoma. Invest Ophthalmol Vis Sci. 2008;49:2799-2805.
41. Jockovich ME, Murray TG, Escalona-Benz E, Hernandez E, Feuer W. Anecortave acetate as single and adjuvant therapy in the treatment of retinal tumors of LH(BETA)T(AG) mice. Invest Ophthalmol Vis Sci. 2006;47:1264-1268.
42. Lee SY, Kim DK, Cho JH, Koh JY, Yoon YH. Inhibitory effect of bevacizumab on the angiogenesis and growth of retinoblastoma. Arch Ophthalmol. 2008;126:953-958.
43. Houston SK, Pina Y, Murray TG, et al. Novel retinoblastoma treatment avoids chemotherapy: the effect of optimally timed combination therapy with angiogenic and glycolytic inhibitors on LH(BETA)T(AG) retinoblastoma tumors. Clin Ophthalmol 2011;5:129-137.
44. Mcevoy J, Flores-Otero J, Zhang J, et al. Coexpression of normally incompatible developmental pathways in retinoblastoma genesis. 2014 in revision.
45. Laurie NA, Donovan SL, Shih CS, et al. Inactivation of the p53 pathway in retinoblastoma. Nature. 2006;444:61-66.
46. Vassilev LT, Vu BT, Graves B, et al. In vivo activation of the p53 pathway by small-molecule antagonists of MDM2. Science. 2004;303:844-848.
47. Elison JR, Cobrinik D, Claros N, Abramson DH, Lee TC. Small molecule inhibition of HDM2 leads to p53-mediated cell death in retinoblastoma cells. Arch Ophthalmol. 2006;124:1269-1275.
48. Brennan RC, Federico S, Bradley C, et al. Targeting the p53 Pathway in Retinoblastoma with Subconjunctival Nutlin-3a. Cancer Res. 2011;71:4205-4213.