







Indications and Considerations For Chromodissection
A number of available dyes can facilitate surgical maneuvers, including ILM peeling.
CHRISTOS HARITOGLOU, MD, FEBO • J. SEBAG, MD, FACS, FRCOphth, FARVO
Advances in our understanding of the anatomy and pathology of the vitreoretinal interface have enabled the development of increasingly successful surgical interventions for vitreomacular disorders.
During surgery, the use of vital dyes helps to visualize barely visible structures, such as the posterior vitreous cortex, pathologic premacular membranes, and the inner limiting membrane of the retina, each of which plays an important role in the pathogenesis of diseases at the vitreoretinal interface.
In recent years, ILM removal has become a widely accepted surgical technique that has resulted in increased success rates because it assures excision of the original source of the pathology — the posterior vitreous.
The intraoperative use of contrast agents has greatly facilitated the complex and challenging maneuver of membrane dissection at the vitreoretinal interface by providing better visualization of this region, minimizing surgical trauma to the underlying retinal nerve fibers.
Although the term “chromovitrectomy” was previously used in this context, this term is inaccurate, because surgeons do not use dyes to perform vitrectomy. Rather, the colored dyes are used to selectively visualize distinct layers at the vitreoretinal interface. The term “chromodissection” is more accurate and appropriate.
Christos Haritoglou, MD, FEBO, is professor of ophthalmology at Herzog Karl Theodor Augenklinik in Munich, Germany. J. Sebag, MD, FACS, FRCOphth, FARVO, is professor of clinical ophthalmology at the Doheny Eye Institute, Los Angeles, CA, and is founding director of the VMR Institute in Huntington Beach, CA. Neither author reports financial interests in products mentioned here. Dr. Sebag’s e-mail address is jsebag@VMRinstitute.com.
The following reviews the anatomy and pathology of the vitreoretinal interface with a special emphasis on the structures that cause vitreomaculopathies requiring membrane dissection for their surgical cure. We will individually analyze the vital dyes employed for chromodissection today.
THE VITREORETINAL INTERFACE
The vitreoretinal interface consists of a complex formed by the ILM of the retina, the posterior vitreous cortex, and an intervening extracellular matrix thought to be responsible for vitreoretinal adhesion (Figure 1A).1

Figure 1. A) Primate (cynomolgus monkey) vitreoretinal interface showing the fibrils of the posterior vitreous cortex, the ILM, and the intervening extracellular matrix. B) Vitreoretinal interface (low magnification) showing the transition from the undulating ILM of the posterior pole (right) to the straight ILM of the peripheral fundus (left) (original magnification = 4,800x).
COURTESY: A) GREGORY HAGEMAN, PHD; B) CHRISTOS HARITOGLOU, MD
The ILM is composed of the proteins laminin, nidogen/entactin, and collagen IV and the proteoglycans perlecan, agrin, and collagen XVIII. Over the entire fundus, the anterior aspect of the ILM has a smooth appearance.
However, the posterior aspect of the ILM varies in structure by location. In the periphery, the posterior aspect of the ILM is smooth and resembles the anterior aspect.
In contrast, in the posterior pole (Figure 1B), the posterior aspect of ILM undulates in an irregular configuration, filling the crevices between underlying retinal glia and nerve fibers.
The posterior vitreous cortex is a 100-to-110-μm–thick layer of densely packed collagen fibrils (Figure 1B). The term “posterior hyaloid face” is often used to refer to this structure, but “hyaloid” is best reserved for the hyaloid artery present during embryogenesis, and “face” should be reserved for the front surface of the vitreous body, often called the anterior hyaloid face.
The lamellar organization of the collagen fibrils of the posterior vitreous cortex results in potential cleavage planes during posterior vitreous detachment, constituting vitreoschisis,2-5 as well as membrane splitting during membrane peel surgery, accounting for some, if not many, failed procedures.
POSTERIOR VITREOUS DETACHMENT
Posterior vitreous detachment is a separation between the posterior vitreous cortex (predominantly type II collagen) and the ILM of the retina (predominantly type IV collagen). This separation occurs when concurrent liquefaction of gel vitreous and weakening of vitreoretinal adhesion.
PVD can be localized, partial, or total (encompassing the posterior pole up to the posterior border of the vitreous base). Clinical studies have estimated the incidence of PVD to be 53% in people age 50 years and older and 65% in those age 65 years and older.6 Autopsy studies have reported incidences of 27% to 51% in the seventh decade of life and 63% in the eighth decade.7
PVD is more common in myopic patients, occurring 10 years earlier than in patients with emmetropia and hyperopia.8 Studies have also found a higher incidence of PVD in women than men, possibly due to postmenopausal hormonal changes.
With aging, aggregation of vitreous collagen fibrils into thick, irregular, visible fibers can induce light scattering, with degradation of contrast sensitivity. This is worse following PVD because of light scattering by the dense collagen fibril network in the posterior vitreous cortex.
Floaters are the most common complaint of patients with PVD, but the root cause of visual dysfunction is a loss of contrast sensitivity, which limited vitrectomy can safely and effectively normalize.9
Anomalous PVD
If the degree of vitreoretinal dehiscence is sufficient to allow for syneresis (collapse), the vitreous body pulls away from the retina without untoward sequelae. However, when insufficient vitreoretinal dehiscence is present, the destabilized, liquefied vitreous cannot pull away cleanly, resulting in anomalous PVD and various sequelae.
When the entire (full-thickness) posterior vitreous cortex separates from the macula but induces peripheral vitreoretinal traction, it induces retinal tears and detachments.
Posterior full-thickness traction can pull on the macula and induce vitreomacular traction syndrome or place traction on the optic disc, exacerbating neovascularization in ischemic retinopathies and inducing vitreous hemorrhage or resulting in vitreopapillary traction syndromes.
PVD with splitting of the posterior vitreous cortex (vitreoschisis) is the first event in the pathogenesis of macular pucker and in some cases of macular hole.
The literature frequently features the term “epiretinal membrane” which is a misnomer. “Epi-” means “adjacent to,” so “epiretinal” could refer to a subretinal locus.
Furthermore, the conditions of relevance are all vitreomaculopathies, so “epiretinal” in imprecise for two reasons. The preferred term is “premacular membrane” because it precisely localizes the membrane to a premacular site.
It is this premacular membrane that must be removed at surgery to treat its untoward effects on the macula. A useful method for assisting in peeling premacular membranes is staining with various dyes, known as chromodissection.
CHROMODISSECTION DURING VITREOUS SURGERY
In recent years, researchers have made significant progress in the field of vitreoretinal surgery. Surgical instruments have been refined and miniaturized from 20-gauge to 23-, 25-, and even 27-gauge in size.
All types of instruments are now available in small gauges that also feature the stiffness required for effective and safe surgical intervention. Optimized wide-angle viewing systems allow for improved access to the far periphery of the eye. Modern surgical machines provide improved pump systems and fluidics.
In addition, the correlations between the clinical aspects and ultrastructural analyses of the vitreoretinal interface have improved our understanding of the pathogenesis of vitreomaculopathies, enhancing their treatment using microsurgical techniques. These insights into ultrastructural characteristics have contributed greatly to the emergence of chromodissection in vitreoretinal surgery.
The primary challenge to effective membrane peeling is that the tissue removed during surgery at the vitreoretinal interface is almost invisible and very delicate to handle due to its thickness in the micrometer range.
Furthermore, the close proximity of important structures, such as the retinal nerve fiber layer, make safe removal of premacular tissue and the ILM even more important to achieving the best possible functional results.
All of this makes chromodissection an important development that not only makes surgery more feasible for vitreoretinal surgeons but also enables the best possible anatomical and functional results for patients.
STAINING SUBSTANCES
Several dyes are in clinical use to visualize the target structure selectively, and all of them have distinct staining properties and characteristics (Table). The surgeon injects the dyes into a fluid- or air-filled globe, and different concentrations are used.
| Dye (concentration) | Premacular membrane | ILM | Vitreous | Mode of application* | Additional comments |
|---|---|---|---|---|---|
| ICG (0.5-0.05%) | --- | Selective +++ | --- | Usually fluid-filled globe | Question of toxicity, off-label |
| Brilliant blue (0.025%) | --- | Selective ++ | --- | Fluid-filled globe (if heavy BBG is used) | Approved in Europe |
| Trypan blue (0.15%) | +++ | (+) | (+) | Fluid- or air-filled globe | Approved in Europe |
| Triamcinolone acetonide | --- | Nonselective (+) | +++ | Fluid-filled globe | No dye, pharmacologic properties |
| Fluorescein | --- | --- | + | Intravitreal, intravenous, or peroral application | |
| *Surgical techniques may vary depending on individual preference. | |||||
Fluorescein provides slight staining of the vitreous, which can sometimes be noted if vitrectomy is performed shortly after angiography.
The dyes currently available for intra-operative visualization of tissues in ophthalmology are indocyanine green, trypan blue, patent blue (Blueron, Fluoron/Geuder), infracyanine green (IfCG, Serb, Paris, France), and brilliant blue (Brilliant Peel, Fluoron/Geuder, Ulm, Germany).
Recently, Dutch Ophthalmic (Zuidland, the Netherlands) released a dual membrane coloring agent containing a combination of Brilliant blue and trypan blue called MembraneBlue Dual, aimed at reducing operating time.
To reduce the operative time and exposure time of the dye on the retinal surface, most of the dyes currently available are offered as heavy solutions. Heavier than water preparations can be achieved by adding deuterium oxide or polyethylene glycol.
Indocyanine Green
Indocyanine green is a tricarbocyanine dye (molecular weight 775 g/M) with a maximum absorption peak at an invisible near-infrared wavelength of approximately 800 nm. Regarding its absorption qualities, ICG may not be an ideal candidate for ILM staining because its maximum absorption is not within the spectral sensitivity of the human eye.10
This limitation implies that relatively high dye concentrations are necessary to achieve sufficient contrast. In addition, the absorption spectrum of ICG overlaps with different types of illumination, posing the risk of phototoxicity to the retina.11-13
ICG is a very unstable molecule and its absorption qualities may vary significantly, depending on the solvent medium and the dye concentration.
Another influence on the absorption spectrum results from progressive aggregate formation with increasing concentration.14 In addition, the light-induced decomposition products have toxic effects on RPE cells.15
Since the introduction of ICG, several studies have emphasized the clinical value of the dye in providing better visualization and allowing for easier and more complete ILM removal (Figure 2).16-18
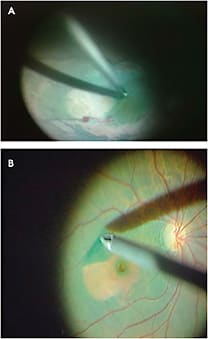
Figure 2. A) Chromodissection of the ILM using ICG; B) Chromodissection with ICG in macular hole surgery.
COURTESY: BERNARDO HENRICH, MD
ICG has not been approved for intraocular injection and represents an off-label use for this indication. The concentration typically injected into the vitreous cavity varies between 0.5% and 0.05%.
Safety Concerns with ICG
Given the photochemical properties of ICG, clinical studies have raised some safety concerns,19,20 although the underlying pathogenic mechanisms are not yet completely understood.
Surgeons have suggested several techniques to reduce the risk of phototoxicity, including reduced dye concentration and less exposure time. They have also covered macular holes with blood or perfluocarbon liquid to prevent dye access to the subretinal space. Experimental studies have addressed the issue of toxicity by attempting to improve the photochemical stability of ICG and alter the absorption qualities.
New cyanine dyes were synthesized, resulting in blue solutions with an intense red fluorescence and an improved absorption maximum of 591 nm, matching the spectral sensitivity of the human eye.21 The fluorescence quantum yield must be sufficiently high to be detected visually (Figure 3).

Figure 3. A new blue dye with a strong fluorescence.
Blue Dyes
Trypan blue. Trypan blue is a large hydrophilic, tetrasulfonated anionic dye with an absorption maximum of 588 nm in water. This dye has been commonly used as a vital stain, including in a wide spectrum of cellular viability tests22,23 and the assessment of arterial endothelial barrier dysfunction.24
In ophthalmology, trypan blue is used in concentrations from 0.0125% to 0.1% to stain the lens capsule to facilitate capsulorrhexis during surgery for mature cataract and for the evaluation of the corneal endothelium of donor tissue before penetrating keratoplasty.25-27 Today, surgeons also use it to assist the preparation of Descemet’s membrane during lamellar keratoplasty.
While the staining properties of trypan blue at the level of the ILM are rather weak, the dye nicely stains premacular membranes (Figure 4).28 The biocompatibility of trypan blue following intraocular use appears very good, with no toxic effects having been reported.
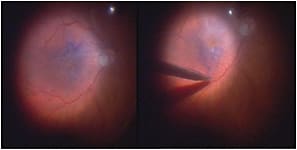
Figure 4. Chromodissection of a premacular membrane using trypan blue.
Brilliant blue. Brilliant blue, also called acid blue or Coomassie, is a blue anionic amino triarylmethane dye. The initial publication on selective ILM staining (Figure 5) during vitreomacular surgery29-31 appeared alongside several experimental studies confirming the excellent biocompatibility of Brilliant blue in cell culture models, animal studies, and electrophysiological studies in humans.32,33
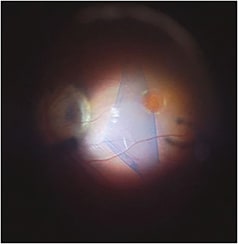
Figure 5. Chromodissection of the ILM using Brilliant blue.
These findings stand in contrast to the reported phototoxicity of ICG, which also represents a selective ILM dye.34 Other dyes of the same class of anionic triarylmethane dyes revealed a similar beneficial safety profile.35 Today, Brilliant blue for ILM staining is approved in many European countries and is commercially available in a concentration of 0.025%.
Because the dye is usually injected into the fluid-filled globe, adjuncts such as deuterium oxide or polyethylene glycol have been added to create a “heavier than water” solution, which facilitates the application of the dye directly over the macular area36 but these additives do not further enhance the contrast effect.37
Both Brilliant blue and ICG can be used to visualize the ILM selectively. Clinical studies investigating the contrast at the retinal surface found better results with ICG than Brilliant blue.38
In addition, both dyes lead to a stiffening of the stained tissue, indicating that additional tissue/dye interactions might occur beyond the staining effect.39 This interaction may explain the rigidity changes in the ILM that appear during vitreomacular surgery and peeling of the tissue. The underlying mechanism of action is possibly related to crosslinking of the collagen fibers of the ILM.
It is important to note, however, that differences exist with regard to the safety profiles of Brilliant blue and ICG. Given the current knowledge on photochemical stability, degradation products, and related toxicity, the safety margin of ICG cannot be determined reliably, limiting recommendations for intraocular use. Nonetheless, ICG is widely used with good clinical results and very few cases of clinical toxicity.
INTRAOPERATIVE STAINING TECHNIQUES
The availability of different dyes with selective staining properties allows for various operative techniques, including sequential “chromodissection” of the vitreoretinal interface.40-42
The “heavier than water” staining substances currently available are usually injected into the fluid filled globe and washed out immediately (Brilliant blue, ICG) or after approximately one minute of exposure time (trypan blue).
In premacular membrane surgery, in which the vitreous is already detached in most cases, especially macular pucker, a reasonable approach is to first peel the premacular membrane without adjuncts, and then visualize the ILM and peel areas where ILM can be detected (single staining).
Alternatively, trypan blue may be used to stain and peel the membrane as a first step, followed by ILM removal using Brilliant blue or ICG (double staining). The surgeon should consider that in most cases the presence of a prominent premacular membrane will render staining of the ILM insufficient should the surgeon apply an ILM dye before removal of the premacular membrane, because the dye has no access to the ILM in these cases.
Nevertheless, injecting an ILM dye before removing premacular membranes will allow for sharp delineation of the borders of the unstained premacular membrane due to a “negative” staining effect.
In macular hole surgery, however, the ILM can be stained without prior removal of premacular tissue as premacular membranes are usually less prominent in eyes with a macular hole. This probably occurs because vitreoschisis in macular holes likely develops posterior to the level of the hyalocytes (in contrast to macular pucker, in which vitreoschisis occurs anterior to the level of hyalocytes), leaving only a thin hypocellular membrane attached to the macula.3,5
TRIAMCINOLONE ACETONIDE AS A CONTRASTING AGENT
Triamcinolone acetonide (TA) may aid in visualizing vitreous during surgery and facilitate its complete removal. (Figure 6). More importantly, it may assist to reliably achieve a complete PVD intraoperatively.
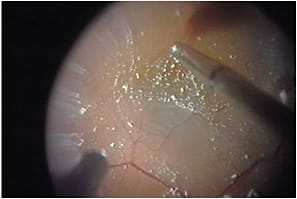
Figure 6. Membrane peeling with triamcinolone acetonide
COURTESY: DANIELE TOGNETTO, MD
The crystals of the TA suspension become entrapped between the collagen fibers and gel structure of the posterior vitreous cortex.43 As a result, TA particles help to determine where the vitreous cortex is still present, especially in cases of vitreoschisis.
A recent report demonstrated that vitrectomy using TA allowed for more efficient removal of the posterior vitreous cortex. TA may also be applied on the retinal surface to assist ILM peeling by providing a contrast between removed and persistent ILM as seen by the presence or absence of TA crystals.44
CONCLUSION
Chromodissection is a surgical technique born of the expansion in knowledge of vitreoretinal interface anatomy and pathology. This useful method to achieve premacular membrane peeling during vitrectomy surgery has contributed to increased success in the surgical cure of vitreomaculopathies.
Several vital dyes are available, each with different properties and applications. Combined use of more than one dye would seem to offer the vitreoretinal surgeon valuable versatility. Although additives produce better contact between dyes and the macula, chromodissection could be improved with methods and instruments to safely apply dyes directly to the surface of the macula.45 RP
REFERENCES
1. Sebag J, Green WR. Vitreous and the vitreo-retinal interface. In: Ryan SJ, ed. Retina, 5th ed. Philadelphia, PA; Saunders; 2012:482-516.
2. Sebag J. Vitreoschisis. Graefes Arch Clin Exp Ophthalmol. 2008;246:329-332.
3. Sebag J, Gupta P, Rosen R, Garcia P, Sadun AA. Macular holes and macular pucker: The role of vitreoschisis as imaged by optical coherence tomography/scanning laser ophthalmoscopy. Trans Am Ophthalmol Soc. 2007;105:121-131.
4. Sebag J. Vitreoschisis in diabetic macular edema. Invest Ophthalmol Vis Sci. 2011;52:8455-8456.
5. Gupta P, Yee KMP, Garcia P, et al. Vitreoschisis in macular diseases. Br J Ophthalmol. 2011;95:376-380.
6. Sebag J. The Vitreous — Structure, Function, and Pathobiology. New York, NY; Springer; 1989.
7. Foos RY. Posterior vitreous detachment. Trans Am Acad Ophthalmol Otolaryngol. 1972;76:480-497.
8. Nguyen N, Sebag J. Myopic vitreopathy — significance in anomalous PVD and vitreo-retinal disorders. In: Midena E, ed. Myopia and Related Diseases. New York, NY; Ophthalmic Communications Society, Inc.; 2005.
9. Sebag J, Yee KM, Wa CA, Huang LC, Sadun AA. Vitrectomy for floaters: prospective efficacy analyses and retrospective safety profile. Retina. 2013 Nov 27. [Epub ahead of print].
10. Langhals H, Haritoglou C. Chemical and spectroscopic aspects of the application of dyes in vitreoretinal surgery. Ophthalmologe. 2009;106:16-20.
11. Yip HK, Lai TY, So KF, Kwok AK. Retinal ganglion cells toxicity caused by photosensitising effects of intravitreal indocyanine green with illumination in rat eyes. Br J Ophthalmol. 2006;90:99-102.
12. Sato T, Ito M, Ishida M, Karasawa Y. Phototoxicity of indocyanine green under continuous fluorescent lamp illumination and its prevention by blocking red light on cultured Müller cells Invest Ophthalmol Vis Sci. 2010;51:4337-4345.
13. Haritoglou C, Freyer W, Priglinger SG, Kampik A. Light absorbing properties of indocyanine green (ICG) in solution and after adsorption to the retinal surface: an ex-vivo approach. Graefes Arch Clin Exp Ophthalmol. 2006;244:1196-1202.
14. Engel E, Schraml R, Maisch T, et al. Light-induced decomposition of indocyanine green. Invest Ophthalmol Vis Sci. 2008;49:1777-1783.
15. Kadonosono K, Itoh N, Uchio E, Nakamura S, Ohno S. Staining of the internal limiting membrane in macular hole surgery. Arch Ophthalmol. 2000;118:1116-1118.
16. Gandorfer A, Messmer EM, Ulbig MW, Kampik A. Indocyanine green selectively stains the internal limiting membrane. Am J Ophthalmol. 2001;131:387-388.
17. Hillenkamp J, Saikia P, Gora F, et al. Macular function and morphology after peeling of idiopathic epiretinal membrane with and without the assistance of indocyanine green. Br J Ophthalmol. 2005;89:437-443.
18. Tsuiki E, Fujikawa A, Miyamura N, Yamada K, Mishima K, Kitaoka T. Visual field defects after macular hole surgery with indocyanine green-assisted internal limiting membrane peeling. Am J Ophthalmol. 2007 Apr;143:704-705.
19. Haritoglou C, Gandorfer A, Gass CA, Schaumberger M, Ulbig MW, Kampik A. Indocyanine green-assisted peeling of the internal limiting membrane in macular hole surgery affects visual outcome: a clinicopathologic correlation. Am J Ophthalmol. 2002;134:836-841.
20. Yam HF, Kwok AKH, Chan KP, Lai TYY, Chu KY, Lam DSC, Pang CP. Effect of indocyanine green and illumination on gene expression in human retinal pigment epithelial cells. Invest Ophthalmol Vis Sci. 2003;44:370-377.
21. Langhals H, Varja A Laubichler P, Kernt M, Eibl K, Haritoglou C. Cyanine dyes as optical contrast agents for ophthalmological surgery. J Med Chem. 2011;54:3903-3925.
22. Sanchez R, Risopatron J, Sepulveda G, Pena P, Miska W. Evaluation of the acrosomal membrane in bovine spermatozoa — effects of proteinase inhibitors. Theriogenology. 2005;43:761-768.
23. Osaka K, Tyurina YY, Dubey PK, et al. Amphotericin B as an intracellular antioxidant. Protection against 2,2-azobis(2,4-dimethylvaleronitrile)induced peroxidation of membrane phospholipids in rat aortic smooth muscle cells. Biochem Pharmacol. 1997;54:937-945.
24. Berman RS, Martin W. Arterial endothelial barrier dysfunction: actions of homocysteine and the hypoxanthine-xanthine oxidase free radical generating system. Br J Pharmacol. 1993;108:920-926.
25. Yetik H, Devranoglou K, Ozkan S. Determining the lowest trypan blue concentration that satisfactorily stains the anterior capsule. J Cataract Refract Surg. 2002;28:988-991.
26. Georgiadis N, Kardasopoulos A, Bufidis T. The evaluation of corneal graft tissue by the use of trypan blue. Ophthalmologica. 1999;213:8-11.
27. Melles GR, de Waard PW, Pameijer JH, Beekhuis WH. Staining the lens capsule with trypan blue for visualizing capsulorrhexis in surgery of mature cataracts. Klin Monatsbl Augenheilkd. 1999;215:342-344.
28. Perrier M, Sebag M. Trypan blue-assisted peeling of the internal limiting membrane during macular hole surgery. Am J Ophthalmol. 2003;135:903-905.
29. Ueno A, Hisatomi T, Enaida H, et al. Biocompatibility of brilliant blue G in a rat model of subretinal injection. Retina. 2007;27:499-504.
30. Enaida H, Hisatomi T, Hata Y, et al. Brilliant blue G selectively stains the internal limiting membrane/brilliant blue G-assisted membrane peeling. Retina. 2006;26:631-636.
31. Enaida H, Hisatomi T, Goto Y, et al. Preclinical investigation of internal limiting membrane staining and peeling using intravitreal brilliant blue G. Retina. 2006;26:623-630.
32. Lüke M, Januschowski K, Beutel J, et al. Electrophysiological effects of Brilliant Blue G in the model of the isolated perfused vertebrate retina. Graefes Arch Clin Exp Ophthalmol. 2008;246:817-822.
33. Remy M, Thaler S, Schumann RG, et al. An in-vivo evaluation of Brilliant Blue G in animals and humans. Br J Ophthalmol. 2008;92:1142-1147.
34. Kawahara S, Hata Y, Miura M, et al. Intracellular events in retinal glial cells exposed to ICG and BBG. Invest Ophthalmol Vis Sci. 2007;48:4426-4432.
35. Haritoglou C, Priglinger SG, Eibl K, et al. Experimental evaluation of aniline and methyl blue for intraocular surgery. Retina. 2009;29:166-173.
36. Haritoglou C, Schumann RG, Kampik A, Gandorfer A. Heavy brilliant blue G for internal limiting membrane staining. Retina. 2011;31:405-407.
37. Henrich PB, Valmaggia C, Lang C, et al. Contrast recognizability during brilliant blue G- and heavier-than-water brilliant blue G-assisted chromovitrectomy: a quantitative analysis. Acta Ophthalmol. 2013;91:e120-e124.
38. Henrich PB, Priglinger SG, Haritoglou C, et al. Quantification of contrast recognizability during brilliant blue G (BBG) and indocyanine green (ICG) assisted chromovitrectomy. Invest Ophthalmol Vis Sci. 2011;52:4345-4349.
39. Haritoglou C, Mauell S, Benoit M, et al. Vital dyes increase the rigidity of the internal limiting membrane. Eye (Lond). 2013;27:1308-1315.
40. Shimada H, Nakashizuka H, Hattori T, et al. Double staining with brilliant blue G and double peeling for epiretinal membranes. Ophthalmology. 2009;116:1370-1376.
41. Schumann RG, Gandorfer A, Eibl KH, Henrich PB, Kampik A, Haritoglou C. Sequential epiretinal membrane removal with internal limiting membrane peeling in brilliant blue G-assisted macular surgery. Br J Ophthalmol. 2010;94:1369-1372.
42. Stalmans P, Freon EJ, Parys-Van Ginderdeuren R, et al. Double vital staining using trypan blue and infracyanine green in macular pucker surgery. Br J Ophthalmol. 2003;87:713-716.
43. Sakamoto T, Ishibashi T. Visualizing vitreous in vitrectomy by triamcinolone. Graefes Arch Clin Exp Ophthalmol. 2009;247:1153-1163.
44. Tognetto D, Zenoni S, Sanguinetti G, Haritoglou C, Ravalico G. Staining of the inner limiting membrane with intravitreal triamcinolone acetonide. Retina. 2005;25:462-467.
45. Meyer CH, Rodrigues EB. A novel applicator for the selective painting of pre-retinal structures during vitreo-retinal surgery. Graefes Arch Clin Exp Ophthalmol. 2005;243:487-489.