







Surgical Management of Suprachoroidal Hemorrhage
Although uncommon, blood in the suprachoroidal space can warrant surgery.
AMAN CHANDRA, MRCSEd, FRCOphth, PhD • TOM WILLIAMSON, MD, FRCS, FRCOphth
Suprachoroidal hemorrhage (SCH) is a rare condition, defined as blood in the suprachoroidal space, consequent to rupture of the short or long posterior ciliary arteries or vortex veins or their tributaries.1,2 Although reports have appeared of spontaneous SCH,3,4 it most commonly presents with a traumatic etiology5 or as complication of ocular surgery.6
Traumatic SCH may occur from multiple blood vessels, both arterial and venous. SCH as a complication of surgery is likely to be secondary to hypotony and may be venous in origin. Animal models have suggested that effusion commences near the posterior pole.2
The clinical presentation may associate with vitreous hemorrhage and occasionally angle closure, as a consequence of the increased posterior-segment pressure. Later, retinal detachment occurs with a high risk of proliferative vitreoretinopathy. The condition appears to associate with “toxic” or hypoxic changes in the retina.
Surgically associated SCH may present perioperatively or on the first day postoperatively. The incidence of SCH after ocular surgery varies, ranging between 0.04% and 1%, for different procedures,3,7-9 depending on ocular and systemic risk factors.
Aman Chandra, MRCSEd, FRCOphth, PhD, is on the faculty of the Vitreoretinal Unit at Royal Victorian Eye & Ear Hospital in Melbourne, Australia. Tom Williamson, MD, FRCS, FRCOphth, is on the faculty of ySt. Thomas’ Hospital in London, United Kingdom. Neither author reports any financial interests related to products discussed here. The authors thank Prof. Gavin Fabinyi, Neurosurgical Department Austin Hospital, Melbourne, for his discussions. The authors hvae no relevant conflicts to disclose. Dr. Chandra’s e-mail is amanchandra@gmail.com.
OUR EXPERIENCE
Our own work on SCH in pars plana vitrectomy has suggested risk factors of male gender, advancing age, use of antiplatelet/anticoagulant drugs, presence of rhegmatogenous retinal detachment or dropped lens fragments, and intraoperative explant application.10
A therapeutic international normalization ratio (INR; a gauge of effect of warfarin) outside of the therapeutic range may be a causative or exacerbating situation, although medication affecting platelets and primary hemostasis have traditionally been thought to have more significant effects on microsurgical hemorrhage.11 We were unable to identify warfarin treatment as an independent risk factor, and we recommend that it be continued through surgery.12
Studies have reported cases of SCH with combined antiplatelet agents, eg, clopidogrel (Plavix, Bristol-Myers Squibb, New York, NY). However, a cohort study did not show increased risk with these agents.13 During vitrectomy, SCH occurs in up to 1% of cases overall, but it is usually limited in area and may be associated with other maneuvers, such as external plombage.14
Retrospective studies have reported lower incidences (0.1 to 0.17%) than prospectively collected data, perhaps because of under-reporting of small bleeds.15,16 Forms from CMS suggested an incidence of 0.5% for SCH.17
It is our belief that intraocular SCH during PPV has a better prognosis than most other causes because earlier recognition and greater control of IOP may limit damage. We have shown that approximately 20% of SCH cases in PPV may end with Snellen vision >20/30, with the most important determinant being preoperative vision (Figure 1, page 66).10,12
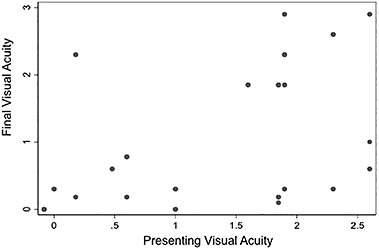
Figure 1. Final visual acuity after suprachoroidal hemorrhage associated with pars plana vitrectomy. Each point represents an individual. The x- and y-axes are visual acuity (LogMAR).
MANAGEMENT
Prevention
SCH is a potentially devastating complication, and its prevention is of paramount importance. The surgical method must reduce the risk. Any surgeon manipulating an eye with an open wound must be extremely careful to reduce the possibility of hemorrhage.
However, it is not entirely clear how this can be done because the mechanisms for the production of this rare complication have not been clearly defined. Logically, some researchers feel that hypotony creates an environment for rupture of a small blood vessel. For this reason, they take steps to reduce wound size and increase wound stability to maintain IOP during surgery.
Even minimally invasive procedures that can cause sudden hypotony (in the prior presence of raised IOP) can lead to SCH, eg, the release of a Supramid suture (S. Jackson, Inc., Alexandria, VA) on a glaucoma implant. The design of surgical equipment, such as vitrectomy and phacoemulsification machinery, can help to optimize stable IOP during surgery.
Other factors may increase the risk of rupture of a blood vessel. The health of the patient’s vasculature and the physical status of the eye may contribute to the risk. As a result, particular patients will require special care.
An example is the highly myopic and arteriopathic patient. In addition, we suspect that changing the shape of the choroid, eg, with the application of external indentation, may also increase of the risk of bleeding, perhaps by fracturing fragile arteriosclerotic blood vessels.
Obviously, the incision of wounds and insertion of sutures close to the suprachoroidal space can either directly injure either intrascleral blood vessels or, by deep penetration, damage the choroidal vasculature, causing hemorrhage.
In particular, the surgeon must take great care to avoid the intrascleral route of the vortex veins, which may or may not be visible but can track for a few millimeters from the insertion of the vein into the sclera.
Intervention
Early recognition during surgery and proactive restriction of further hypotony by closing wounds and raising IOP certainly limit progression of the hemorrhage. The surgeon should remember, before performing any intervention that might reduce IOP again, to try to provide sufficient time for the thrombus in the vessel wall to form, plugging the rupture in the blood vessel and preventing further hemorrhage.
For the anterior-segment surgeon, recognition of the complication occurs late, because these surgeons often only see the hemorrhage with loss of the red reflex, which may explain the presentation of “expulsive” hemorrhage after anterior-segment surgery (rarely seen in vitrectomy).
The posterior-segment surgeon has direct visualization of the retina and greater opportunity to see the hemorrhage early. Employing smaller wounds, the vitreoretinal surgeon is in a position to stabilize and increase IOP quickly, which helps to limit the spread of the hemorrhage and may explain the better visual outcomes in these situations.10
SURGICAL DILEMMAS
If SCH occurs perioperatively, should we take immediate action? Obvious actions include stabilization of wounds and increasing the IOP, but should a surgeon attempt immediate evacuation?
To prevent further bleeding, it is important that a clot forms that will plug the rupture in the blood vessel wall. Some clinicians have thought that small bleeds require a two- to five-minute duration.18 However, because a thrombus is also forming in the suprachoroidal space during this period, the opportunity to remove hemorrhage fluid is being lost.
As a result, immediate evacuation of SCH perioperatively is difficult to achieve effectively: evacuate too early, and the rupture in the blood vessel may not be blocked off and may bleed further; wait too long, and the hemorrhage in the suprachoroidal space will have solidified.
Even if the surgeon gets the timing correct, immediate evacuation runs the risk of dislodging the thrombus in the blood vessel and creating more hemorrhage.
Proceeding With Caution
A more conservative approach is not to evacuate during the primary operation but to wait a few weeks to allow for thrombolysis of the SCH and closure of the rupture in the blood vessel wall by healing.
The eye can often clear hemorrhage surprisingly effectively, sometimes with spontaneous resolution over weeks, which is another reason to wait. Our experience has been that some SCHs will clear more rapidly than others.
For example, the highly myopic eye, which is at greater risk for SCH, appears to spontaneously clear more easily than the emmetropic eye.
Intuitively, one can envisage the thinner sclera allows for easier egress of hemolysis blood. Identifying whether an effusion component to the hemorrhage exists is important, for example, in a post-trabeculectomy situation, which will also contribute to easier egress of fluid and resolution.
Thrombolysis of whole blood theoretically takes 10-20 hours. However, thrombolysis of large bleeds can be much slower. For example, total resolution of thrombosis in all deep-vein thrombosis cases occurs in 25% of patients within one month and in 40% in three months.19 Animal models of liquefaction of thrombi in the suprachoroidal space have suggested that one to two weeks are necessary for this to occur.20
However, in the presence of a large “spherical” clot, this time seems to increase, perhaps because plasmin cannot penetrate the large thrombus, and clinically, two to three weeks are required to significantly reduce the size of the solid thrombus in the suprachoroidal space.
Such a time frame for thrombus hemolysis and, consequently, surgery also occurs in neurosurgical hemorrhages of venous origin — particularly subdural hemorrhages. Although small series of earlier interventions in SCH have appeared,21 most reports agree with a short delay.22,23
An indicator of the need to intervene early is whether the macula is free of hemorrhage or not. This will usually require ultrasonography to determine, when direct visualization cannot be achieved. A macula with an SCH under it is likely to suffer from toxicity or hypoxia, which is a reason to intervene early. SCH will usually break through the retinal and choroidal tissues, creating vitreous hemorrhage and obscuring the view of the retina as a result.
Subsequent Surgeries
At secondary surgery, our technique and that of others24 is to insert an anterior-chamber maintainer first to increase IOP. This is effective even in phakic or pseudophakic eyes. The surgeon then exposes the sclera under the SCH to create a small sclerotomy of 1-2 mm. He or she should ensure to place the incision posteriorly enough to reach the hemorrhage cavity but anterior to any vortex veins.
The surgeon should allow extrusion of the liquid from the cavity by increasing the pressure internally. He or she can reduce approximately two-thirds to three-quarters of the volume of the cavity by this method (Figure 2).
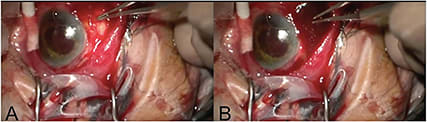
Figure 2. Drainage of SCH via sclerostomy. A) Sclerostomy site. B)Sclerostomy site opened allowing drainage of blood.
However, complete resolution is unlikely. Small pieces of clot may block the sclerotomy, and the surgeon should gently extrude these or extract them using a vitreous cutter external to the orifice. Eventually no more fluid will come out, and the surgeon can convert to a vitrectomy with pars plana infusion, allowing for clearance of the vitreous cavity and examination of the hemorrhage internally.
The surgeon can insert perfluoro-N-octane (PFO) (“heavy liquid”) to encourage more fluid hemorrhage toward the sclerotomy.25 It can be very satisfying to reduce a choroidal hemorrhage in this way, greatly debulking the elevation.
The experience of trying to remove a residual clot by creating a scleral window to directly visualize the suprachoroidal space has not been worthwhile, in our experience. The clot has the consistency of cottage cheese and cannot be removed in one piece, as a fresh clot sometimes can.
Using a vitrectomy cutter to shave down the “cottage cheese” is not particularly effective. As a result, we recommend allowing this to clear itself over a time course of weeks or even months.
Recent Developments
The inability of proteins to penetrate the thrombus suggests that injection of tissue plasminogen activator is unlikely to help, although it has been described in a case report26 and may be worth investigating, especially once the clot has reduced in size.
Recently, Rezende et al have suggested that transconjunctival, sutureless, trocar-based sclerostomy drainage using 20-gauge ports can be successful.27 Such techniques have yet to be replicated.
For tamponade of the vitreous cavity, a noncompressible fluid is preferable to minimize the extent of any new bleeds. Balanced salt solution or oil is a better medium than gas.24,28 The latter is, of course, compressible, and the surgeon should only use it if confident that no further bleeds will occur.
Postoperative follow-up should be undertaken with great care. The risk of further hemorrhages is unclear and variable, depending on the initial etiology. If rebleeding occurs, the ocular prognosis worsens.
CONCLUSION
SCH is a devastating situation with visual outcomes similar to those of postoperative endophthalmitis. As we discussed, the prognosis most likely depends on the underlying etiology and severity of the SCH. Those with small bleeds not involving the macula have a better chance of spontaneous or successful surgical resolution, and they are most likely to do well. RP
REFERENCES
1. Manschot WA. The pathology of expulsive hemorrhage. Am J Ophthalmol. 1955;40:15-24.
2. Beyer CF, Peyman GA, Hill JM. Expulsive choroidal hemorrhage in rabbits. A histopathologic study. Arch Ophthalmol. 1989;107:1648-1653.
3. Chak M, Williamson TH. Spontaneous suprachoroidal haemorrhage associated with high myopia and aspirin. Eye (Lond). 2003;17:525-527.
4. Chandra A, Barsam A, Hugkulstone C. A spontaneous suprachoroidal haemorrhage: a case report. Cases J. 2009;2:185.
5. Wolter JR. White thrombi in massive subchoroidal haemorrhage: indicators of the site of its origin and of the mechanism of its control. Br J Ophthalmol. 1985;69:303-306.
6. Wolter JR. Expulsive hemorrhage during retinal detachment surgery. A case with survival of the eye after Verhoeff sclerotomy. Am J Ophthalmol. 1961;51:264-266.
7. Speaker MG, Guerriero PN, Met JA, Coad CT, Berger A, Marmor M. A case-control study of risk factors for intraoperative suprachoroidal expulsive hemorrhage. Ophthalmology. 1991;98:202-209.
8. Wang LC, Yang CM, Yang CH, et al. Clinical characteristics and visual outcome of non-traumatic suprachoroidal haemorrhage in Taiwan. Acta Ophthalmol. 2008;86:908-912.
9. Cantor LB, Katz LJ, Spaeth GL. Complications of surgery in glaucoma. Suprachoroidal expulsive hemorrhage in glaucoma patients undergoing intraocular surgery. Ophthalmology. 1985;92:1266-1270.
10. Chandra A, Xing W, Kadhim MR, Williamson TH. Suprachoroidal hemorrhage in pars plana vitrectomy: risk factors and outcomes over 10 years. Ophthalmology. 2014;121:311-317.
11. Pandolfi M. Hemorrhages in Ophthalmology. Stuttgart, Germany; Georg Thieme Publishers; 1979.
12. Chandra A, Jazayeri F, Williamson TH. Warfarin in vitreoretinal surgery: a case controlled series. Br J Ophthalmol. 2011;95:976-978.
13. Mason JO 3rd, Frederick PA, Neimkin MG, et al. Incidence of hemorrhagic complications after intravitreal bevacizumab (avastin) or ranibizumab (lucentis) injections on systemically anticoagulated patients. Retina. 2010;30:1386-1389.
14. Narendran N, Williamson TH. The effects of aspirin and warfarin therapy on haemorrhage in vitreoretinal surgery. Acta Ophthalmol Scand. 2003;81:38-40.
15. Tabandeh H, Sullivan PM, Smahliuk P, Flynn HW Jr, Schiffman J. Suprachoroidal hemorrhage during pars plana vitrectomy. Risk factors and outcomes. Ophthalmology. 1999;106:236-242.
16. Sharma T, Virdi DS, Parikh S, Gopal L, Badrinath SS, Mukesh BN. A case-control study of suprachoroidal hemorrhage during pars plana vitrectomy. Ophthalmic Surg Lasers. 1997;28:640-604.
17. Stein JD, Zacks DN, Grossman D, Grabe H, Johnson MW, Sloan FA. Adverse events after pars plana vitrectomy among medicare beneficiaries. Arch Ophthalmol. 2009;127:1656-1663.
18. Hattersley PG. Activated coagulation time of whole blood. JAMA. 1966;196:436-440.
19. Janssen MC, Wollersheim H, Haenen JH, van Asten WN, Thien T. Deep venous thrombosis: a prospective 3-month follow-up using duplex scanning and strain-gauge plethysmography. Clin Sci (Lond). 1998;94:651-656.
20. Lakhanpal V. Experimental and clinical observations on massive suprachoroidal hemorrhage. Trans Am Ophthalmol Soc. 1993;91:545-652.
21. Pakravan M, Yazdani S, Afroozifar M, Kouhestani N, Ghassami M, Shahshahan M. An alternative approach for management of delayed suprachoroidal hemorrhage after glaucoma procedures. J Glaucoma. 2014;23:37-40.
22. Jin W, Xing Y, Xu Y, Wang W, Yang A. Management of delayed suprachoroidal haemorrhage after intraocular surgery and trauma. Graefes Arch Clin Exp Ophthalmol. 2014 Jan 29. [Epub ahead of print]
23. Lakhanpal V, Schocket SS, Elman MJ, Nirankari VS. A new modified vitreoretinal surgical approach in the management of massive suprachoroidal hemorrhage. Ophthalmology. 1989;96:793-800.
24. Quiroz-Mercado H, Garza-Karren CD, Roigmelo EA, Jimenez-Sierra JM, Dalma-Weiszhausz J. Vitreous management in massive suprachoroidal hemorrhage. Eur J Ophthalmol. 1997;7:101-104.
25. Desai UR, Peyman GA, Chen CJ, et al. Use of perfluoroperhydrophenanthrene in the management of suprachoroidal hemorrhages. Ophthalmology. 1992;99:1542-1547.
26. Kunjukunju N, Gonzales CR, Rodden WS. Recombinant tissue plasminogen activator in the treatment of suprachoroidal hemorrhage. Clin Ophthalmol. 2011;5:155-157.
27. Rezende FA, Kickinger MC, Li G, Prado RF, Regis LG. Transconjunctival drainage of serous and hemorrhagic choroidal detachment. Retina. 2012;32:242-249.
28. Feretis E, Mourtzoukos S, Mangouritsas G, Kabanarou SA, Inoba K, Xirou T. Secondary management and outcome of massive suprachoroidal hemorrhage. Eur J Ophthalmol. 2006;16:835-840.