







FOCUS ON…
OCT Ups Its Game With Swept-source
RENÉ LUTHE, SENIOR ASSOCIATE EDITOR
At Vitreous Retina Macula Consultants of New York, Michael Engelbert, MD, PhD, reports that spectral-domain OCT (850 nm) has become routine in many clinical scenarios for the enhanced depth imaging of the choroid it offers. But technology inevitably moves on, and while the physicians there remain happy with the quality of imaging SD-OCT delivers, a recent advance has enabled them to bypass to the weak points SD inevitably includes.
BEYOND SPECTRAL DOMAIN
The DRI (Deep Range Imaging) OCT-1 Atlantis (Topcon Medical, Oakland, NJ, www.topconmedical.com) features swept-source OCT. The technology utilizes longer wavelength (1,050 nm) compared to SD-OCT (850 nm), which means better tissue penetration. “This allows not only for simultaneous representation of the retina and choroid, but also the vitreous in excellent detail,” Dr. Engelbert explains. “It also gets around some of the problems imaging high myopes and patients with cataract.”
And because swept-source is also much faster than SD-OCT — the Atlantis has an imaging speed of 100,000 A scans/sec, compared to 25,000 A scans/sec for the Topcon 3D OCT-2000 — patients experience improved comfort. The greater speed also eliminates saccadic motion artifact when a large number of averaged images are necessary.
“Image acquisition is a matter of seconds, even if a high number of line scans is acquired for averaging,” Dr. Engelbert says. He reports that line scan takes about one second, and the 3D cube or crosshair approximately five seconds.
Though the Atlantis is not FDA approved yet, his practice has had the opportunity to use it in clinical studies since 2010. “I have a particular interest in imaging the vitreous and vitreoretinal interface, and the swept-source cannot be beat there,” Dr. Engelbert says.
SHARPER IMAGES, SIMULTANEOUSLY
Swept-source OCT allows the clinician to avoid certain trade-offs necessary in spectral-domain devices. In SD-OCT, a separate enhanced depth scan has to be acquired in order to represent vitreous, retina, and choroid simultaneously. “Though this has become a standard feature on some machines, it still requires taking another scan that will show a great choroidal image, but at the expense of the image quality of the vitreous and vitreoretinal interface,” Dr. Engelbert explains.
“Conversely, one can trick the spectral-domain OCT into imaging the vitreous with pretty good detail, but a high number of averages is necessary, and the resultant scan time makes maintaining fixation difficult for many patients, he says. Involuntary eye movements then lead to ‘ghosting’ artifacts. The swept-source gets around this by virtue of its speed.”
THE SPECIFICS
The depth of tissue penetration and the 12-mm scan width the Atlantis offer make a big difference in the clinic, Dr. Engelbert notes. “These have allowed us to scan an area of about 18 mm by 18 mm covering the posterior pole — that is, about halfway up to the equator.” He reports being able to image approximately 2.6 mm into the vitreous from the retinal surface. “That has allowed us not only to clarify the relationships between some elusive liquefied vitreous spaces (Figure 1), but also to start grading vitreous degeneration (Figure 2).1 I believe that characterizing the state of not only the vitreoretinal interface, but also the vitreous itself may be helpful in predicting the response to pharmacological vitreolysis. This is clearly an area where better prognostic indicators are direly needed,” he says.
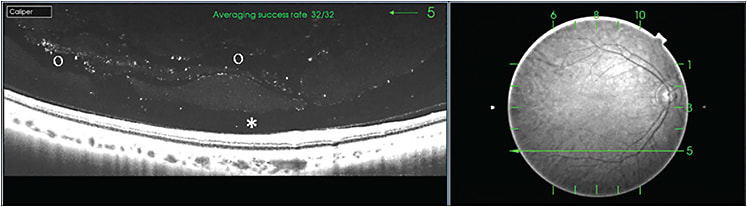
Figures 1 and 2. SS-OCT visualized degenerative vitreous changes. The premacular bursa (*) can be seen overlying the macula in the horizontal line scan on the left, corresponding to the green arrow in the infrared image on the right. Several degenerative cleavage layers (O) can be seen adjacent to the bursa.
IN THE PRACTICE ENVIRONMENT
Given the speed of swept-source, the more generous scan width, and its elimination of the need for separate choroidal or vitreous scans, Dr. Engelbert expects the DRI OCT-1 will improve patient flow once the FDA approves it for the US market. Its advantages extend to the medical staff as well, he says. His practice’s photographic staff, all experienced with either the 3D OCT or other prior-generation OCTs, was almost immediately comfortable with the Atlantis. “It’s really not very different from taking an OCT image with any other machine,” he notes.
As for finding space in your practice, Dr. Engelbert concedes that the Atlantis requires more than the earlier-generation Topcon 3D-OCT. “The computing power needed for the amount of data and speed at which it is acquired make external hardware necessary and the footprint larger.” The system is comprised of the OCT device and an external desktop with its monitor and keyboard.
Dr. Engelbert notes that practices may be reluctant to make the outlay required for another OCT, particularly when physicians can obtain most of the information that typically need in day-to-day clinical practice with spectral domain platforms. “However, the Atlantis’s speed and patient comfort and the ability to scan large areas of the retina, plus its ability to visualize the vitreous, make it unique in the current market,” he says. RP