







CONTROVERSIES IN CARE
Vitrectomy for Floaters
EDITED BY MICHAEL COLUCCIELLO, MD
The entopic sensation of floaters (Figure), the gray patches that may temporarily obscure vision, can affect perceived quality of life in some individuals. Vitreous collagen reorganization and liquefaction (which occur in all individuals over time) results in aggregation of collagen fibrils, liquefaction of the gel (vitreous synchysis), and collapse (vitreous syneresis) of vitreous “away” from the retina (posterior vitreous detachment).1
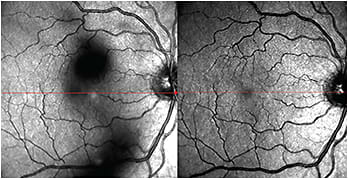
Figure. Scanning laser ophthalmoscope image (left) of focal floaters in the right eye. When these floaters enter the optical axis, degradation of contrast sensitivity occurs due to light scattering. Postoperative SLO (right) demonstrates clearing of floaters after minimally invasive vitrectomy.
COURTESY: J. SEBAG, MD
These phenomena cause the symptoms of floaters and are almost universal with time. The subjective appreciation of the sudden appearance of floaters is common after a PVD, the most common etiology. Floaters are also a common symptom of vitreous synchysis, and fibrous aggregation occurs in young people, related to myopia and myopic vitreopathy.
Michael Colucciello, MD, is a clinical associate in the Department of Ophthalmology at the University of Pennsylvania School of Medicine in Philadelphia and a retina specialist practicing with South Jersey Eye Physicians in Moorestown, NJ. He reports no financial interests in products mentioned in this article. Dr. Colucciello’s e-mail is michael@macula.us.
Frank H. Koch, MD, is head of the Department for Vitreous and Retinal Surgery at the Eye Clinic of the J.W. Goethe University Hospital in Frankfurt, Germany.
J. Sebag, MD, FACS, FRCOphth, FARVO, is professor of clinical ophthalmology at the Doheny Eye Institute, Los Angeles, CA, and is founding director of the VMR Institute in Huntington Beach, CA.
Despite vitreous synchysis and syneresis occurring in almost everyone, only some individuals perceive an effect on the quality of their lives. This fact highlights that many patients become accustomed and adapt to floaters, but others report distressing symptoms interfering with many activities of daily living.
A MYSTERY
There must be an explanation, but no studies have been undertaken to identify why. Because no pathologic effects on the eye result from vitreous synchysis and syneresis (assuming no anomalous PVD2 with an associated retinal tear or other pathology3), observational management of the patient with floater symptomatology is undertaken with the expectation that accommodation and adaptation will occur.
To date, this approach has certainly been a useful, conservative manner to manage these individuals. However, some patients continue to report adverse effects of floaters on their quality of life, and they seek help, sometimes desperately.
A prospective study was undertaken via a questionnaire given to 266 consecutive patients with a history of floaters to evaluate the effects of floaters on individuals’ quality of life.4,5 The results seemed to show that floaters have a negative impact on quality of life, comparable to ocular and systemic diseases.
This study (performed in Singapore) indicated that the “utility values” (quality of life) of floaters were equal to those with AMD and similar to those with diabetic retinopathy and glaucoma. In this study, floaters affected quality of life in a way similar to angina, “mild” stroke, colon cancer, and asymptomatic HIV infection.
WORTH THE RISK?
Incredibly, this study found that these patients were willing to take an 11% risk of death and 7% risk of blindness, and they were willing to trade off 1.1 years out of every 10 years of their remaining lives to rid themselves of the symptoms of floaters!
Because floaters may negatively affect the quality of life in certain individuals, “treatment” has been sought. However, the majority of patients who undergo Nd:YAG vitreolysis for treatment of their floaters will not be aided by that intervention.6
Pars plana vitrectomy can rid the eye of floaters, but it can have side effects. The greatest risks of PPV are retinal tears at the time of surgery and cataract formation in the near term after the surgery.7,8
These consequences are perhaps alleviated by a surgical approach wherein subtotal vitrectomy is accomplished: no vitreous detachment is induced, and at the conclusion of the case, the superior trocars are extracted with nonhollow probes within them (to mitigate against vitreous incarceration in the sclerotomies).
POSSIBLE COMPLICATIONS
Leaving an intact posterior vitreous cortex, however, can lead to an anomalous vitreous separation later, associated with a macular pucker or other manifestations of anomalous PVD. In addition, a later complete posterior vitreous separation can be associated with recurrent floater symptoms. Further, in phakic patients, the anterior vitreous is kept intact behind the lens to guard against cataract-inducing oxygenation of the lens after vitrectomy.9
In consideration of these issues, how shall we counsel patients with floaters who feel they are negatively impacting the quality of their lives? This month, we are fortunate to have the expert commentary of Drs. Jerry Sebag and Frank Koch.
REFERENCES
1. Sebag J. The Vitreous — Structure, Function, and Pathobiology. New York, NY: Springer; 1989.
2. Sebag J. Anomalous posterior vitreous detachment — a unifying concept in vitreo-retinal diseases. Graefes Arch Clin Exp Ophthalmol. 2004;242:690-698.
3. Sebag J. Vitreous anatomy, aging, and posterior vitreous detachment. In: Besharse J, Dana R, Dartt DA, eds. Encyclopedia of the Eye. Vol. 4. Oxford, United Kingdom; Elsevier; 2010:307-315.
4. Wagle AM, Lim WY, Yap TP, et al. Utility values associated with vitreous floaters. Am J Ophthalmol. 2011;152:60-65.
5. Sebag J. Floaters and the quality of life [editorial]. Am J Ophthalmol. 2011;152:3-4.
6. Delaney YM, Oyinloye A, Benjamin L. Nd:YAG vitreolysis and pars plana vitrectomy: surgical treatment for vitreous floaters. Eye (Lond). 2002;16:21-26.
7. Tan HS, Mura M, Lesnik Oberstein SY, et al. Safety of vitrectomy for floaters. Am J Ophthalmol. 2011;151:995-998.
8. Wilkinson CP. Safety of vitrectomy for floaters — how safe is safe? [editorial]. Am J Ophthalmol. 2011;151:919-920.
9. Sebag J, Yee KM, Wa CA, et al. Vitrectomy for floaters: prospective efficacy analyses and retrospective safety profile. Retina. 2013 Nov 27. [Epub ahead of print]
The Case for Vitrectomy
J. SEBAG, MD, FACS, FRCOphth, FARVO
We began performing vitrectomy for floaters approximately 15 years ago when the use of YAG lasers to treat floaters was promoted on the East Coast. Patients from California traveled there to be treated, but some returned miserable, worse than they were before.
The results with vitrectomy in these patients were excellent, and the patients were happy. Yet the degree of surgery required with 20-gauge instruments and the methods employed at that time seemed too invasive to offer to more patients complaining of floaters.
With the advent of sutureless 25-gauge vitrectomy, attitudes began to change. When a study appeared demonstrating how we in the medical profession have underestimated the negative impact of floaters on quality of life, the approach to these patients became more respectful and open minded.1
A Change in Perception
What was lacking, however, was an objective means to quantify floaters, either structurally or functionally. It was the brilliant Alfredo Sadun, MD, PhD, at the Doheny Eye Institute who reasoned that light scattering by vitreous opacities would not only cast shadows perceived by patients as floaters, but it could also degrade contrast sensitivity.
Finally, a way to distinguish between patients who were truly disturbed by floaters and not just obsessing and over-reacting was available. Using the Freiburg Acuity Contrast test (FrACT), we found a reproducibility of 92% and diminution in floater patients of 67% (P<.01).2
But how could we help these patients? Could vitrectomy be undertaken safely enough? A critical analysis of vitrectomy techniques was undertaken, and a minimally invasive procedure was designed, using highly beveled sclerotomies and nonhollow probes for cannula removal to prevent vitreous incarceration, preserving vitreous behind the lens to lessen cataracts and not inducing surgical PVD to mitigate retinal breaks.2
Results So Far
To date, we have treated 95 patients in this manner. Considerably diminished contrast sensitivity was common preoperatively. Following surgery, every single patient measured had normalized contrast sensitivity, which has remained normal for more than a year so far (P<.01). Patient satisfaction was documented using the NEI VFQ-36, and it improved by 30% (P<.001).3
No cases of endophthalmitis or retinal detachment occurred. One patient experienced vitreous hemorrhage that cleared spontaneously after two weeks. In patients who did not have a PVD preoperatively and in whom PVD was not induced surgically, a PVD developed in two cases (13 months and four months postoperatively), and macular pucker developed in one case. Surgery corrected the problems in all three cases.
Cataract surgery was necessary an average of 13 months after vitrectomy in 14 of 60 (23%) phakic eyes, which compared favorably with the 50% to 76% incidence previously reported.4,5 The mean age was 63 years, and no patients younger than 53 years needed cataract surgery.
Looking Ahead
In summary, this experience has been remarkable, primarily because of the happiness it has created in these genuinely unhappy people. The key is to define “genuine” unhappiness, which has been made easier by measuring contrast sensitivity and VFQ.
In collaboration with engineers in New York, we are currently developing an objective means to quantify floaters by ultrasound, to have an objective quantitative structural correlate of the functional deficit induced by floaters.
REFERENCES
1. Sebag J. Floaters and the quality of life [editorial]. Am J Ophthalmol. 2011;152:3-4.
2. Wa C, Sebag J. Safety of vitrectomy for floaters. Am J Ophthalmol. 2011;152:1077.
3. Sebag J, Yee KM, Wa CA, et al. Vitrectomy for floaters: prospective efficacy analyses and retrospective safety profile. Retina. 2013 Nov 27. [Epub ahead of print]
4. Yee KM, Wa C, Nguyen J, et al. Reducing post-vitrectomy cataracts. Invest Ophthalmol Vis Sci. 2014;55:ARVO E-Abstract 2205.
5. Tan HS, Mura M, Lesnik Oberstein SY, Bijl HM. Safety of vitrectomy for floaters. Am J Ophthalmol. 2011;151:995-998.
Strategies for Patient Selection for Floater Removal
FRANK KOCH, MD
As noted in the literature,1 many patients are willing to risk blindness, and some have even said that death would be acceptable to alleviate the symptoms of floaters and improve quality of life. “Floaterectomy” is a viable option, and the potential benefits could outweigh the risks.
Nevertheless, prior to removing clinically significant “floaters” from patients’ eyes, surgeons should develop strategies to select a qualified group of patients and adhere to a precise routine considering the individual patient’s eye.
Some Recommendations
I recommend the following routine. All patients record their perceived personal and individual type of floater pattern on paper or using a scanner. Effects on quality of life, visual quality, and well being and the character of vision disorders are distinctively recorded pre- and postoperatively with a visual function questionnaire (NEI VFQ-25 test or a customized floater questionnaire, designated the FFQ-22 test).2-4
Patients have their degree of vision impairment recorded with a test to detect their quality of vision before and after surgery.5 Central vision analysis allows the patient and the doctor to determine the effects of the floaters and the patients’ quality of vision under various contrast conditions.
When considering “floaterectomy,” the physician should carefully evaluate the efficacy of a one-step, single incision site, 23-gauge core vitrectomy or a one-step two incision site, 23-/26-gauge procedure for the safe and efficient removal of clinically significant opacities.
This minimally invasive “floaterectomy” procedure is performed in phakic and pseudophakic eyes (aseptic conditions, topical or peribulbar anesthesia, balanced salt solution, head-mounted indirect ophthalmoscope). Some patients may require laser treatment for equatorial degeneration before the removal of their floaters.1
Data From My Practice
In my experience, 112 patients’ floaters were removed with one-site or two-site PPV (no PVD); 3.6% had two-site, three-port PPV for revision (plus PVD induction). The lenses were unaffected in 92% (follow-up of two years). Retinal detachment occurred in 0.9%. Ninety-nine percent of patients reported improvement in their quality of life, and Sloan visual acuity improved in 85%.
Although the drawing of floaters on paper revealed well the degree of transparency loss, the geometry of floaters was best recorded with a scanner. The central visual acuity test values (including all those under mesopic and glare conditions) revealed a remarkable improvement in vision for those eyes (50%) that suffered from dense floaters centered on the visual axis.
Our minimally invasive PPV approach was quick and accurate and was characterized by fewer side effects (eg, cataract development) and fewer complications (eg, retinal detachment). On rare occasions, one eye may need to be revised with two-site or three-port PPV.6-8 Performing all tests before and after “floaterectomy” and using the minimally invasive techniques mentioned above contributed substantially to our patients’ satisfaction and convinced them to proceed with the removal of potentially symptomatic vitreous opacifications in their fellow eyes. RP
REFERENCES
1. Sebag J. Floaters and the quality of life. Am J Ophthalmol. 2011;152:3-4 e1.
2. Bradley EA, Sloan JA, Novotny PJ, Garrity JA, Woog JJ, West SK. Evaluation of the National Eye Institute visual function questionnaire in Graves’ ophthalmopathy. Ophthalmology. 2006;113:1450-1454.
3. Orr P, Rentz AM, Margolis MK, et al. Validation of the National Eye Institute Visual Function Questionnaire-25 (NEI VFQ-25) in age-related macular degeneration. Invest Ophthalmol Vis Sci. 2011;52:3354-3359.
4. Henkel V, Mergl R, Kohnen R, Maier W, Möller HJ, Hegerl U. Identifying depression in primary care: a comparison of different methods in a prospective cohort study. BMJ. 2003;326:200-201.
5. Gutstein W, Sinclair SH, North RV, Bekiroglu N. Screening athletes with Down syndrome for ocular disease. Optometry. 2010;81:94-99.
6. Dayan MR, Jayamanne DG, Andrews RM, Griffiths PG. Flashes and floaters as predictors of vitreoretinal pathology: is follow-up necessary for posterior vitreous detachment? Eye (Lond). 1996;10:456-458.
7. de Nie KF, Crama N, Tilanus MA, Klevering BJ, Boon CJ. Pars plana vitrectomy for disturbing primary vitreous floaters: clinical outcome and patient satisfaction. Graefes Arch Clin Exp Ophthalmol. 2013;251:1373-1382.
8. Fujii GY, De Juan E Jr, Humayun MS, et al. Initial experiences using the transconjunctival sutureless vitrectomy system for vitreoretinal surgery. Ophthalmology. 2002;109:1814-1820.