







Preparing for Lost Revenue Due to Elimination of Consult Codes
Rosie Taulbee, FACMPE
When the Centers for Medicare and Medicaid Services eliminated consult codes in 2010, many specialty practices had multiple areas of disruption in their daily processes and, more importantly, loss of revenue. As the manager of a practice's retina division, it was important for me to monitor this change and document the impact to both the physicians and the consultant from the accounting firm. Analysis allowed us to project if changes needed to be implemented for office overhead or if we needed to consider moving the retinal physicians to their own corporation.
RAISING THE ALERT FLAG
Medical practices must be aware of the coming changes to the 5010 electronic claims filing standard to be implemented on October 1, 2012 and the ICD-10 Diagnostic Codes slated for the year 2013. The multiple areas that require change will be difficult to accomplish in the medical practice in the time frame allotted. The current 17,000 ICD-9 codes for all medical diagnoses will be replaced with 141,000 codes. Involvement with accountable care organizations will also experience significant impact with these coding changes for future reimbursement.
In our practice, the changing CPT procedure consult codes created drastic effects. The physicians, certified coders and billing staff needed specific directions about what codes were eliminated by CMS to document changes for any contracted Medicare Advantage plans that chose to follow Medicare guidelines. Both the in-office billing encounter forms used to document the claim transmission charge and the electronic medical record needed “alerts” to pop up or identify eliminated codes for the physicians. Our practice had three insurance carriers in addition to CMS that did not allow consult codes.
Staff keying charges or electronic claims scrubbing were needed to catch errors and ask the physician or certified coder to correct the procedure code prior to submitting to the insurance carrier for reimbursement. Initial error rates increased, since the coding information was received at a slow pace from various insurance carriers via their newsletters, snail mail and e-mail or by the practices' internal staff verifying coding changes on each insurance carrier's Web site.
ANALYZING THE CHANGES
Each month, I documented three areas: (1) The total procedures performed and corresponding dollar charges by CPT code for each retinal physician. (2) Actual revenue from all insurance carriers associated with those charges by physician for the month. (3) A separate tally of the days worked in the office by each physician to verify that the procedures performed and associated charges were not distorted due to vacation, holiday or attendance at continuing medical education days away from the office. These categories were then compared to the prior year's performance when the consult codes were still allowed by all insurance carriers.
When the consult codes 99244 and 99245 were eliminated, our retinal physicians used the appropriate code 99204 and 99205 for new patients that came from referring physicians outside of the practice's Tax-ID corporation. The established codes 99214 and 99215, if appropriate, were billed for patient referrals within the same Tax-ID corporation or on rare occasion when the patient returned within the three-year period for evaluation and management as opposed to a “consult.”
Table 1. A Comparison of Charge Dollars in 2009 and 2010 For Two Retina Specialists in the Midwest*
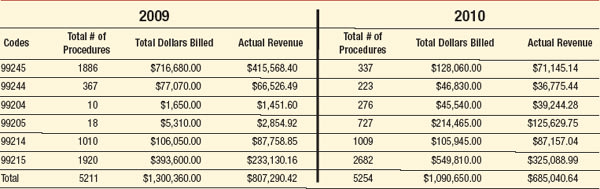
*The collection rate remained at 62% both years, but there was a $122,249.78 decline in revenue from 2009 to 2010 after the elimination of consult codes.
DECLINING REVENUE
Table 1 reveals the $209,710 decrease in charge dollars for the 2010 year for two retina specialists located in the midwest. The number of patient visits in the facility increased by 43 patients in the 2010 year and three additional days were spent working in the outpatient offices. The collection process for the corporation was not altered due to the coding change. At year-end in both 2009 and 2010, the collection rate for these procedures remained at 62%. The revenue received for these procedures from traditional Medicare and the Medicare Advantage plans revealed a loss of $122,249.78 from the 2009 year when consult codes were utilized.
This example is used to help readers understand the time, effort and costs associated with minimal changes to CPT consult codes. These changes were easily accommodated by the practice billing software, since it simply involved codes that already existed in the practice management software system, and blocking or adding coding alerts to their electronic medical record system.
THE ROAD AHEAD
The impending ICD-10 diagnosis changes will require, at a minimum, the following:
• Physician education about selecting the accurate diagnosis code. Hopefully there will be ample time for physician training through conferences, seminars and on-demand webinars by specialty.
• Training for billing staff keying additional codes—regardless of whether the practice is using EMR or entering charges in the office.
• Recertification for all Certified Professional Coders.
• Precertification of the new diagnosis codes must be completed before procedures are performed in order for the practice to receive revenue for the codes.
• Updated billing staff and coder forms. Software for the electronic formats will also need to load on the codes and the crosswalk procedure verification related to the diagnosis.
• Software updates for the clearinghouse that transmits the diagnosis on claims to the insurance carrier.
• Insurance company software system updates to incorporate new codes and crosswalking to the procedure for the payment amount. They also must clarify if the reimbursement amounts will be different for each code.
• Electronic medical record downloads of the new diagnosis codes.
• Expanded management reports involving diagnosis codes for the practice to compensate for the increased volume of codes.
• Updated laboratory intake, billing and reporting systems for any labs receiving specimens for testing.
• Upgraded hospital scheduling systems for surgery, pre-certification of procedures with diagnoses, and claims transmission to accept the ICD-10 codes.
If two retina physicians lost $122,249.78 with the elimination of consult codes, what will the associated reimbursement for ICD-10 cost the entire healthcare system? Prepare yourself by planning for these changes. RP
| Rosie Taulbee, FACMPE, is board certified in medical practice management and is a fellow in the American College of Medical Practice Executives. She may be reached at 513-353-9079 or taulbeerosie@hotmail.com. This article was compiled with data from the Retina Division, located in Ohio. |