







Microperimetry and Pituitary Adenoma
Benign tumors can present as retinal symptoms.
FEDERICO M. RATHSCHULER, MD
Pituitary adenoma is the most common tumor that involves this important gland.1,2 Usually beginning as a small, encapsulated lesion within the sella, it may grow in several directions. While endocrine dysfunction (amenorrhea, galactorrhea, erectile dysfunction and/or infertility) are the most common manifestations, in a discrete percentage of patients, visual, sensory or ocular motor dysfunction occur as primary symptoms.3
Microperimetry is a noninvasive procedure that allows for exact topographic correlation between fundus loci and their light sensitivity by stimulating selected retinal locations under infrared light examination. Here the author describes a case of pituitary adenoma with nonspecific ocular signs discovered from a microperimetric exam.
A healthy man, 62 years old, was referred to my office in June 2008, complaining of light metamorphopsia in his left eye lasting two months. His right eye was asymptomatic. He had no previous ophthalmic history of note.
On examination, retinoscopy disclosed a mildly myopic refractive error in both eyes; corrected visual acuity was 20/20 in the right eye and in 20/25 in the left. Reading acuity was normal in both eyes. Amsler Test showed minimal metamorphopsia in the left eye. Slitlamp examination was normal in the right eye but revealed an initial lens opacity (grade 1) in the left eye. Extraocular movements were full; there was no strabismus or nystagmus.
Retinal examination showed minimal RPE anomalies in both eyes. Optic disc and retinal vascular arcades were normal. Central 10° microperimetry showed a normal appearance in the right eye, except for an isolated light sensibility reduction in the extreme inferonasal area and a scattered reduction of sensitivity in the left eye (Figure 1). Fluores cein angiography showed minimal RPE anomalies in both eyes. The presence of minimally symptomatic metamorphopsia in the left eye should have been related to the presence of rare pigment alterations in the foveal region.
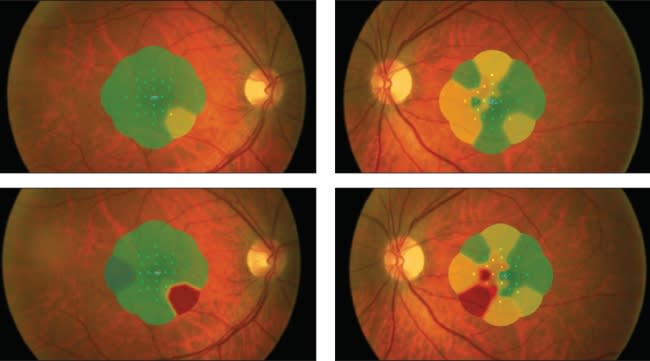
Figure 1. First microperimetry exam (top): Central 10° microperimetry showed a normal appearance in right eye, except for an isolated light sensitivity reduction in the extreme inferonasal area examined and a scattered reduction of sensitivity in his left eye. Second microperimetry exam (bottom): Central 10° microperimetry showed a large decrease in sensitivity where it was just minimally reduced previously in both eyes and a clear appearance of ominous defect.
Two months later, the patient complained of decreased visual acuity and increased metamorphopsia in the left eye. Corrected visual acuity was 20/20 in the right eye and 20/30 in the left. Reading acuity was normal in the right eye and slightly reduced in the left. Slit-lamp, retinal, optic disc and vascular arcade examinations were unchanged.
Central 10° microperimetry showed a high decrease in sensitivity where it was just minimally reduced previously in both eyes and a clear appearance of ominous defect (Figure 1).
Octopus 1-2-3 (Haag-Streit, Koeniz, Switzerland) perimetry confirmed the suspicions of an incomplete, superior bitemporal quadrantanopsia (Figure 2), and magnetic resonance imaging disclosed the presence of a pituitary adenoma. The patient had the unique presentation of subtle discomfort with a slight reduction of visual acuity in his left eye where moderate lens opacity and minimal RPE anomalies were present, possibly misleading the diagnosis. Amsler test, performed during the examination, was not as clear as microperimetry in revealing the presence of bitemporal visual field defects. RP
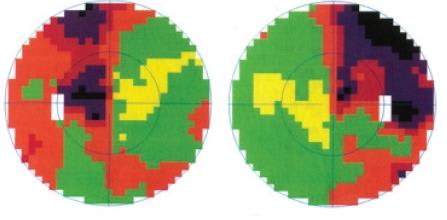
Figure 2. Octopus 1-2-3 perimetry confirmed the suspicion of an incomplete, superior, bitemporal quadrantanopsia.
REFERENCES
1. American Cancer Society. Detailed guide: pituitary tumor. American Cancer Society Web site. http://www.cancer.org/docroot/cri/cri_2_3x.asp?dt=61. Accessed January 10, 2008.
2. Ezzat S, Asa SL, Couldwell WT, et al. The prevalence of pituitary adenomas: a systematic review. Cancer. 2004;101:613-619.
3. Melmed S, Keliberg D. Anterior pituitary. In: Melmed S, Kronenberg H, Polonsky K, Larsen PR, eds. Williams Textbook of Endocrinology.11th ed. Philadelphia, PA: Elsevier; 2007.
4. Midena E. Perimetry and the Fundus: An Introduction to Microperimetry. Thorofare, NJ: Slack; 2007.
| Federico M. Rathschuler, MD, practices at Studio Oculistico Rathschuler in Genoa, Italy. He reports no financial interest in any products mentioned in this article. Dr. Rathschuler can be reached via e-mail at frath@fastwebnet.it. |