







Clinical Experiences With a New Vitrectomy System
Panelists discuss the newest features of the Bausch & Lomb Millennium Vitrectomy Enhancer — including some remarkable data on flow rate and duty cycle — and how this system compares with others.
Carl C. Awh, MD: Our panel consists of a number of experienced surgeons, all of whom have used the Bausch & Lomb Millennium Vitrectomy Enhancer (MVE) and comparable competitive systems.
Let's begin with a discussion of vitrectomy cutters in general. Dr. Heier, what do you seek from your vitrectomy cutter?

|
"The new cutters, especially the MVE system, have tremendously altered our approach. The improved flow rates and cutting efficiency, as well as the absence of flexibility in the instruments, allow us to maneuver and attack tissue anteriorly. Our ability to tackle all types of cases from the smaller incision vitrectomy has radically changed our approach to surgery." —Jeffrey S. Heier, MD |
Jeffrey S. Heier, MD: In general, we look for efficient cutting of the vitreous, minimal movement of adjacent tissues, and adequate flow. After evaluating a first-generation 25-gauge system, we were somewhat hindered by the flexibility of the instruments, although we really liked being able to perform small-incision vitrectomy. Working almost exclusively with fellows, who perform 70% to 80% of our cases, we moved away from 25-gauge for a while because of that difference in the instruments.
The new cutters, especially the MVE system, have tremendously altered our approach. The improved flow rates and cutting efficiency, as well as the absence of flexibility in the instruments, allow us to maneuver and attack tissue anteriorly. Our ability to tackle all types of cases from the smaller incision vitrectomy has radically changed our approach to surgery. Previously, about 20% of our vitrectomies were small-incision surgeries. Now, as many as 80% are small-incision vitrectomies.
CUTTER EFFICIENCY
Dr. Awh: Dr. Chow, what variables affect how we determine the flow of tissue through a vitrectomy cutter?
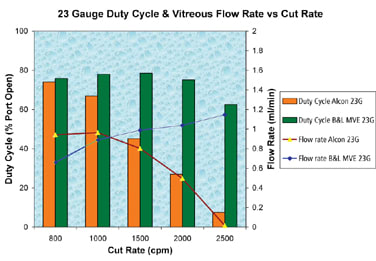
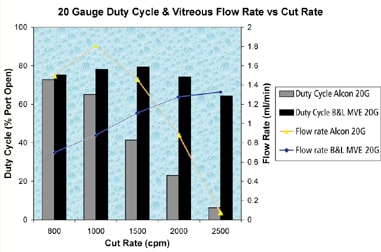
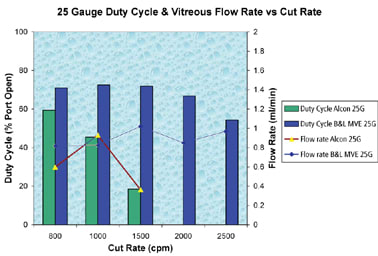
David R. Chow, MD: Essentially, we look at vacuum, cut rate, port size and duty cycle. With older-generation pneumatic cutters, as we increased the cut rate, we experienced a significant drop in flow. The main reason for this was a decrease in the duty cycle or the amount of time the cutter port remained open with each cutting cycle. With the new MVE cutter, as we cut faster — and it is most noticeable with the 25-gauge cutter — the flow rate is maintained. Data obtained from the Eye Concepts Laboratory at Doheny Retina Institute at the University of Southern California seem to suggest we can maintain flow rates with this 25-gauge cutter up to about 2500 cuts per minute (cpm) without a significant loss in flow between 1500 cpm and 2500 cpm.
| Rewriting the Rules | |
|---|---|
| It appears that the rules we were taught many years ago — that flow decreases with increasing cut rates — applied only to a pneumatic cutter that had a decreasing duty cycle with increasing cut rate. Now, we have a cutter that can maintain a high duty cycle with high cut rates. I think one of reasons for this astonishing flow is the viscoelastic nature of vitreous as it moves through the cutter and the line. My opinion is that because we are taking much smaller bites of vitreous, these small pieces of vitreous at a given vacuum level move with less friction and, therefore, more rapidly through the tubing. That's why a higher cut rate at a given level of vacuum produces higher flow. — Carl C. Awh, MD |
|
|
|
Data courtesy of Eye Concepts Laboratory at Doheny Retina Institute at the University of Southern California.
What this means for surgeons, and what's amazing about this new cutter, is that we can use the highest cut rate available almost all of the time. In fact, it simplifies our lives because the only variable we need to adjust is the vacuum. For a core vitrectomy, where we want efficiency, we can achieve a high flow level by using high vacuum levels while on the surface of the retina, or we can reduce the vacuum to achieve low flow rates and precision.
Dr. Awh: Until the advent of the technical advances found in the MVE system, the performance of pneumatic cutters was limited. Traditional pneumatic cutters, the ones used by virtually all other commercially available vitrectomy systems, have an unavoidable decrease in flow with increasing cut rate. In fact, repeated tests have demonstrated that the flow through most "high speed" pneumatic cutters at maximum cut rates is so low as to be almost useless. These performance characteristics became even more apparent upon the introduction of the B&L "Lightning" electric cutter, which, at the time of its introduction, was the only high-speed cutter able to maintain a 50% open duty cycle at all cut rates. This made 25-gauge surgery truly practical.
What's amazing with the MVE cutter is that changes in its internal design allow it to maintain an open duty cycle even at the highest cut rates. The graphs above (see "Rewriting the Rules") show that not all pneumatic cutters are equal, and that there's something very special about this pneumatic cutter that allows us to sustain high flow rates while maintaining a safer, more effective high cut rate.
Dr. Stanga, with the MVE cutter, do you find you need to vary cut rate to achieve your clinical goal? Or do you tend to use a higher cut rate most of the time?
Paulo E. Stanga, MD: We tend to use it at a high cut rate. In our experience, we have not needed to vary the cut rate so much. I was highly impressed by the efficiency of the cutter.
Dr. Awh: Another advantage of the MVE is that this new cutter technology adapts to the existing Millennium system, so we do not need to purchase an entirely new machine to have the latest cutter performance.

|
"With the new MVE cutter, as we cut faster, … the flow rate is maintained. Data … seem to suggest we can maintain flow rates with this 25-gauge cutter up to about 2500 cuts per minute (cpm) without a significant loss in flow between 1500 and 2500 cpm." —David R. Chow, MD |
GAUGE PREFERENCES
Dr. Awh: We have been discussing 25-gauge cutters specifically, but I believe these comments relate to all gauges. Dr. Stanga, what gauge cutter do you typically use?
Dr. Stanga: We have a large fellowship program in Manchester, where the fellows perform many surgeries with and without supervision, so we do not use 25-gauge because of the flexibility of the instruments. We are impressed with the 20-gauge MVE and the 23-gauge MVE.
Dr. Awh: How do you decide which gauge to use for a given case with the MVE cutter?
Dr. Stanga: We are gradually converting to 23-gauge for most cases because of advantages not only for the surgeon, but also for the patient's comfort. By using a single gauge, we avoid needing to discuss what system to use with the theater staff. The theater nurses automatically open the pack for 23-gauge and set the system. Hopefully, that's what we will be using for all of our cases in the future.
Dr. Awh: Dr. Blinder, you perform a lot of 23-gauge surgery. Is 23-gauge your preferred system?
Kevin J. Blinder, MD: When 25-gauge first became available, we made the transition as a group, but many of us were disappointed because of the flexibility of the instrumentation. When the 23-gauge technology became available, most of us converted to 23-gauge vitrectomy because of the easier transition and the more rigid instrumentation.
I have been so impressed with the MVE that I went back to the 25-gauge cutter with the MVE system, and I have seen a remarkable improvement in cutter efficiency. The flow is unbelievable. I think it eliminates the need for the 3D technology that Alcon introduced. You can vary aspiration while maintaining the cut rate at its highest level, which is a nice innovation.

|
"What's amazing with the MVE cutter is that changes in its internal design allow it to maintain an open duty cycle even at the highest cut rates." —Carl C. Awh, MD |
Until the introduction of the B&L 23-gauge cutter, I was doing a hybrid procedure, using the MVE 25-gauge cutter with the 23-gauge trocar system, so I would have the option of using 23-gauge instrumentation. I have used the new B&L 23-gauge system and have found it to be a nice 1-step set-up with an excellent 23-gauge cutter.
Dr. Heier: When we started using the B&L 25-gauge MVE cutter, we found that the flexibility was outstanding. It is just like using a 23-gauge instrument, yet it goes in and out through the trocar system easily. It is a great combination.
Dr. Chow: The main complaint about 25-gauge cutters, as we all know, has been the increased flexibility when rotating the eye, making access to the periphery difficult. What was startling to me with the new MVE cutter is that there is unquestionably a significant increase in stiffness. For surgeons who like 25-gauge vitrectomy and are happy with their experience with it, I think there are three very good reasons they will love this cutter:
1) Increased stiffness
2) Increased cut rate of 2500 cpm
3) Improved flow rates at the full cut rate.
Dr. Awh: Dr. Rizzo, you have had a great deal of experience and have published many articles about 25-gauge vitrectomy, but more recently you have been using 23-gauge vitrectomy. How are you using the MVE system?
Stanislao Rizzo, MD: I started using 25-gauge instrumentation in 2001 and then changed to 23-gauge. With the older systems — and I have used four different brands — I noticed a great deal of traction when operating near the retina. I think the big change is the sharpening of the system. I see less traction with the MVE than with any of the other systems I use. I believe the probe material is completely different. It cuts the vitreous more effectively with each bite of the cutter.

|
"We tend to use [the MVE cutter] at a high cut rate. In our experience, we have not needed to vary the cut rate so much. I was highly impressed by the efficiency of the cutter." —Paulo E. Stanga, MD |

|
"I have been so impressed with the MVE that I went back to the 25-gauge cutter with the MVE system, and I have seen a remarkable improvement in cutter efficiency. The flow is unbelievable. … You can vary aspiration while maintaining the cut rate at its highest level, which is a nice innovation." —Kevin J. Blinder, MD |
I think soon there will be no need for 23-gauge because our concerns about flexibility, flow and the efficiency of the probe will disappear. Why would I want to make a larger incision on the sclera if 25-gauge is just as efficient or even more efficient? I probably will transition to 25-gauge, and I will reserve 20-gauge for when I need to use silicone oil.
Dr. Awh: I share a similar mindset, although I acknowledge that there are some advantages to the stiffness of larger-gauge forceps and scissors, particularly for doctors who are teaching fellows.
In terms of removing vitreous and manipulating the eye during more straightforward cases, however, the 25-gauge MVE cutter is much better than first-generation cutters, in my opinion. I believe one of the reasons 23-gauge gained a foothold so quickly is that most surgeons experienced 25-gauge vitrectomy with a "first-generation" pneumatic cutter that had such poor flow characteristics that they were quick to abandon it. Now that this new generation of pneumatic cutters provides tremendous flow in 25-gauge, I encourage surgeons to revisit 25-gauge to see if some of their initial objections are no longer valid.
Dr. Blinder: Previously, we mentioned needing 20-gauge for silicone oil injection. We actually can inject silicone oil now through 23-gauge ports very easily. This is an advantage of 23-gauge over 25-gauge, versus the need to go back to 20-gauge vitrectomy. Also, I have not been able to perform a good dropped nucleus lensectomy with 25-gauge, whereas using 23-gauge, I can remove 90% of lenses with just the vitrector.
|
"I think the big change is the sharpening of the system. I see less traction with the MVE than with any of the other systems I use. I believe the probe material is completely different. It cuts the vitreous more effectively with each bite of the cutter." —Stanislao Rizzo, MD |
Dr. Awh: Dr. Chow has designed a thin-walled cannula that allows silicone oil injection through a 25-gauge wound. It is somewhat slower, but if you want to keep the integrity of your 25-gauge wounds, it is a viable option.
Dr. Chow: A couple of products are available now for 25-gauge silicone oil injection. It is definitely doable.
Dr. Awh: I have done several cases where I have removed an entire dropped lens with the 25-gauge MVE cutter. Have any of the panelists removed dropped lenses or portions of dropped lenses with the 25-gauge cutter?
Dr. Heier: I have done a number of cortical fragments and relatively soft nuclear fragments with the 25-gauge MVE cutter, and the procedures have gone smoothly. You have to remember, all of our 23-gauge right now is really with the 25-gauge cutter. We would prefer to do these cases with the small incision and not disrupt conjunctiva, because I think many of these complicated cataract cases go on to become glaucoma cases. I prefer to disrupt conjunctiva as little as possible.
Dr. Awh: It will be interesting to observe how the preferences of retina specialists change with the availability of improved technology like the MVE.
Dr. Heier: In preparing for today's discussion, I looked at results from the 2007 Preferences and Trends Survey of the American Society of Retina Specialists (ASRS). (Editor's note: ASRS members may view survey results online at http://www.asrs.org). For a straightforward epiretinal membrane (ERM), 60% of surgeons use a small incision 80% to 100% of the time. That is a significant increase from 2006, so I think there clearly is a transition from 20-gauge to 23-gauge. It is definitely easier to take fellows from 20 to 23 than it is to go straight from 20 to 25.
Dr. Stanga: I fully agree with that. Many fellows who come through our program find it much easier to use 23-gauge rather than 25-gauge.

|
"Now that this new generation of pneumatic cutters provides tremendous flow in 25-gauge, I encourage surgeons to revisit 25-gauge to see if some of their initial objections are no longer valid." —Carl C. Awh, MD |
WOUND CONSTRUCTION
Dr. Awh: Let's discuss wound construction using 23-gauge vs 25-gauge. Dr. Stanga, what is your experience?
Dr. Stanga: We did a study, which we presented as a poster at the 2006 meeting of the American Academy of Ophthalmology.1 Using third-generation time-domain optical coherence tomography (OCT), which is the technology that was available at that time, we looked at wounds created with a straight entry with 25-gauge. We found that the scleral wound remained open 5 to 6 weeks after the surgery. That is a concern, especially because of the risk of endophthalmitis or hypotony. With the MVE 23-gauge, I believe there's not much reason for concern with a 1-step approach. I'm very happy about the wound. I can sleep again.
Dr. Awh: Who is using a single-step 23-gauge system?
Dr. Rizzo: I use both. The disadvantage of the 2-step system is that sometimes there is some blood under the conjunctiva, and you cannot see the first incision. That is the reason why some surgeons now use a 1-step 23-gauge system. I think wound construction in 2 steps is better, however, because you have an MVR blade in your hand to make the first incision.
Dr. Awh: I think a blade makes a better wound than a needle does, whether it is solid or hollow core. What's more, as Dr. Stanga mentioned in his studies, the 25-gauge wounds do not close as quickly as an equivalent-sized blade wound, but because the wounds are so small in diameter, wound construction is less critical. As Dr. Rizzo mentioned, adapting to the 2-step system is somewhat more difficult, so it is reasonable for the companies to try to make a 1-step system that improves 23-gauge ease of entry. Who has tried the new 23-gauge 1-step system that comes with the MVE?
Dr. Chow: I have used it. What is nice about it is that this 23-gauge system behaves, looks and feels nearly identical to the previous and current B&L 25-gauge trocar cannula system. For surgeons who have been using the 25-gauge trocar cannula insertion, this newer 23-gauge trocar cannula will give them the same experience.
Regarding wound design, as many of you know, my last 500 cases have been 20-gauge sutureless. I think the only reason I can create a 20-gauge sutureless wound is that I create a really flat wound with an MVR blade. I think the key element for Dr. Rizzo is that he has an MVR blade in his hand. There's no question that blade design affects wound construction. The bigger the wound is, the more important that becomes.

|
"I have done a number of cortical fragments and relatively soft nuclear fragments with the 25-gauge MVE cutter, and the procedures have gone smoothly." —Jeffrey S. Heier, MD |
POLYIMIDE CANNULA
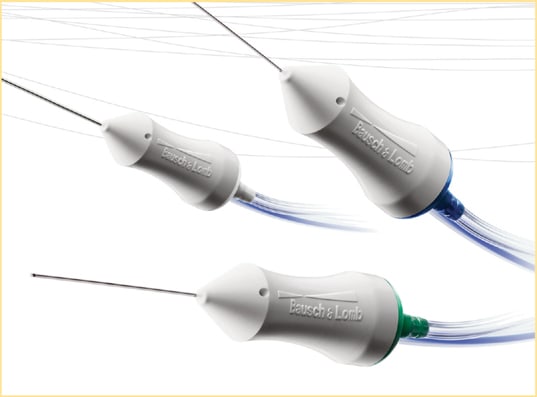
Dr. Awh: One of the nice features of the 23-gauge MVE Entry Site Alignment System (Figure 1) is the polyimide cannula. These cannulas are similar to those in the 25-gauge system, and I think they have some advantages over metal cannulas. They are not as heavy, so they do not fall off the needle prior to insertion. They seem to have better friction in the sclerotomy, so they are less likely to slip out during surgery. Have others noticed any differences with the MVE trocar-cannula system?
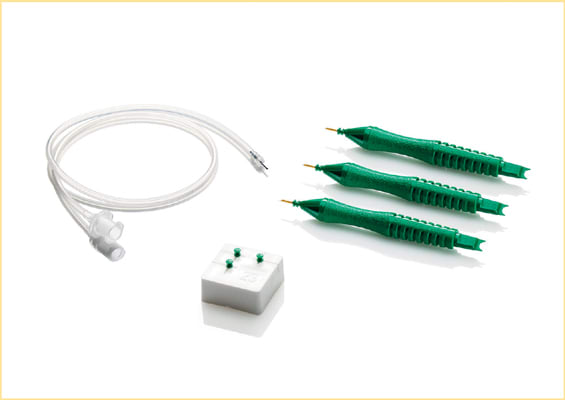
Figure 1. Bausch & Lomb Millennium Vitrectomy Enhancer 23-Gauge Entry Site Alignment System

|
"What is nice about the MVE 23-gauge I-step system is that it behaves, looks and feels nearly identical to the previous and current B&L 25-gauge trocar cannula system. For surgeons who have been using the 25-gauge trocar cannula insertion, this newer 23-gauge trocar cannula will give them the same experience." —David R. Chow, MD |
Dr. Blinder: I have not had a cannula come out with the MVE. I think polyimide has another advantage. I do not get the tunnel vision effect from the light pipe as I am trying to vitrectomize anteriorly on the side of the light pipe. I can illuminate through the cannula and see the anterior vitreous space more easily.
Dr. Chow: That is a great point. That is something I have shown in videos, and it is a tip I teach our fellows. When you put a light pipe in a polyimide cannula, it diffuses the light, and you create what I call a "poor man's chandelier." Obviously, you cannot do that with a steel cannula.
Dr. Awh: I agree. With an opaque steel cannula, particularly the longer ones necessary for oblique 23-gauge incisions, it is noticeably more difficult to illuminate the peripheral retina near the cannula through which the light pipe is introduced. Dr. Rizzo, you have used these various systems. Do you see any advantage in having polyimide for the cannulas in 23-gauge?
Dr. Rizzo: There is an advantage because the shape of the wound at the end of the surgery is better with the polyimide cannula. The metal cannula can enlarge the wound, but it is more resistant.
Dr. Heier: For us, there's another issue because we are operating in an ambulatory surgery center, and the metal trocars can be reused. From a cost perspective, that can be somewhat of an advantage. As we reuse them, however, we can have issues with instrument entry. Small burrs, for example, can hinder instruments going in and out, so we have to replace them occasionally.
Dr. Awh: I believe you are not permitted to reuse these sorts of instruments in Europe. Is that correct?
Dr. Stanga: We are not permitted to reuse them in the UK. As Dr. Rizzo mentioned, I think the polyimide cannula is gentler on the lips of the wound, and it does not seem to come off the wound as easily as the other ones.
Dr. Awh: It is an interesting combination of features. The polyimide cannula conforms to the wound a bit and, therefore, does not stretch the wound as much, and its surface properties create better friction within the sclerotomy tunnel so it does not pull out quite as easily.
Dr. Chow: One other point with the cannula design — and I was a fairly big proponent of this — is that the cannula has been lengthened. The original 25-gauge cannulas were designed to go from point A to point B across the sclera in a perpendicular, straight-in manner. Now, we are creating angled wounds, and, obviously, the space between point A and point B on a long angled wound is much longer. So, to me, lengthening the cannula is an important issue as surgeons start moving to longer angled wounds to create enough internal clearance of the cannula. Hopefully, lengthening the cannula will reduce risks, such as having the cannula go suprachoroidal.

|
"One of the nice features of the 23-gauge MVE Entry Site Alignment System is the polyimide cannula. … These cannulas have some advantages over metal cannulas. They are not as heavy, so they do not fall off the needle prior to insertion. They seem to have better friction in the sclerotomy, so they are less likely to slip out during surgery." —Carl C. Awh, MD |
Improved Ergonomics In the past, many surgeons were willing to use the heavier, larger electric handle because of the benefits of improved duty cycle. Now, we can use the familiar smaller and lighter pneumatic cutter and obtain the superior performance provided by an optimized duty cycle. — Carl C. Awh, MD |
Dr. Awh: This cannula is somewhat longer than any other 23-gauge cannula, which allows the surgeon to make as long and as flat a sclerotomy wound as possible. Dr. Rizzo, you have taught about wound construction. Do you agree that a longer cannula is an advantage?
Dr. Rizzo: Yes. I agree completely, because the longer the wound construction, the better the integrity of the wound at the end of surgery. This is one of the secrets of successful surgery.
WOUND CLOSURE
Dr. Awh: For those of you who have used the 23-gauge MVE 1-step system, what is your experience with wound closure? Does the system allow you to create watertight wounds? How often do you need to suture your 23-gauge sclerotomies?
Dr. Rizzo: With this 23-gauge system, I never put sutures at the end of the surgery now.
Dr. Chow: The wounds have been reliable, but with a caveat being that because of my 20-gauge sutureless background, almost all of my cases are "sutureless vitrectomy." I put an air bubble in all my cases, so I think I am getting a little advantage of that air tamponade across the wound. I would be curious to hear from other panelists who are not using an air tamponade on sutureless vitrectomy routinely. What is your experience with the 23-gauge wound?
Dr. Blinder: I use an air bubble as well because I want to see if air is leaking through the wound. I have used the Alcon 1-step and was disappointed with it. I think the B&L 1-step has a better seal than the Alcon 1-step and comes close to the Dutch Ophthalmic 2-step system.
Dr. Awh: Will you switch to the 1-step system now that you have this one from B&L with pre-loaded cannulas?
Dr. Blinder: We'll probably use both at different centers, but I think it will be easier to sit by and watch the fellows perform the 1-step.

|
"I think the polyimide cannula is an advantage. I do not get the tunnel vision effect from the light pipe as I am trying to vitrectomize anteriorly on the side of the light pipe. I can illuminate through the cannula and see the anterior vitreous space more easily." —Kevin J. Blinder, MD |
Dr. Stanga: We just have to get used to seeing the eye sink a bit into the orbit.
Dr. Awh: With any needle-type trocar, regardless of the cannula material, there will be more friction when introducing a bigger trocar.
I do not routinely inject air at the end of sutureless cases, and in my limited experience with 23-gauge cases, I have had them seal very nicely in fluid-filled eyes. I have not had to suture any of them. I prefer to test the eye's pressure fluid-filled, and I inject some air at the end with a 30-gauge needle if I am not confident the wounds are sealed. However, I do not inject air routinely. Is everyone else putting in air routinely?
Dr. Heier: I use just fluid. When we pull the first two cannulas, the infusion is clamped, and we see if the eye is maintaining pressure. Then we watch when we pull the third one to make sure it is maintaining pressure, as well. We do not routinely put in air.
Dr. Rizzo: I always put in air at the end of the case. It may be a coincidence, but in a paper about endophthalmitis published in Retina in 2008, those cases with endophthalmitis had fluid in the vitreous chamber.2 Now, I prefer to put in air at the end of my surgery.
Dr. Heier: Regillo and colleagues at Wills Eye Institute in Philadelphia looked at their 25-gauge cases, air vs no air, angled vs straight. They found that fluid-filled eyes did much better with angled wounds. They saw no difference in terms of postoperative complications.3
Dr. Awh: The advent of 23- and 20-gauge sutureless surgery has made me think more about wound construction and has given me a new understanding of the value of oblique sclerotomy wounds. As I have stated often, oblique wounds are not necessary for most 25-gauge cases. The wounds are small enough that they are watertight independent of entry angle.
I have learned, however, that the real benefit of oblique 23- and 20-gauge sutureless wounds is not simply the greater length of the wound, but that the edges of an oblique wound can be somewhat reapproximated with blunt pressure after the cannula is removed. I now press down over the scleral tunnel with a blunt forceps. With an oblique wound, I often can see the oval wound edges flatten and close. This technique is essential for 23- and 20-gauge sutureless vitrectomy, and can be helpful in certain 25-gauge cases, as well. As I mentioned, only in the rarest cases do I need to inject an air bubble. I generally leave the eye fluid-filled, and these eyes maintain excellent pressure at the end of surgery.
Dr. Stanga: I prefer to leave the eye fluid-filled if I am performing posterior pole surgery or dealing with an ERM or a hole. However, if I am rotating the eye quite a lot to access the periphery and I'm stretching the wounds by rotating the eye, I feel more confident to fill the eye with air.
CUTTER SAFETY AND VERSATILITY
Dr. Awh: We have discussed the improved flow and touched on the safety of the cutter. I would like to discuss that topic further. Dr. Rizzo mentioned that he observes less traction near the retina with the MVE cutter. Dr. Rizzo, do you think that allows you to do more with this cutter than you can with other types of vitreous cutters?
Dr. Rizzo: Yes, definitely. For example, I use the new cutter with its fixed 2500 cpm cut rate and the foot-controlled vacuum switch for a core vitrectomy and when I am near the retina. I also use the cutter for diabetes cases with fibrovascular membranes or traction.
Dr. Blinder: I have reduced my use of scissors by using the smaller-gauge vitrector. It is a nice advantage. The less you introduce instruments into and out of the eye, the less likely you are to have peripheral tears.
Dr. Awh: One of the features I have always liked about 25-gauge is that the cutter tip is so small and delicate. I can manipulate it nicely between the retina and membranes, and I can dissect quite closely to the retinal surface without having to switch to scissors. I can use bimanual techniques with the cutter, as well. Sometimes, I find myself using chandelier illumination with a pick or forceps in one hand and my cutter in the other to dissect a challenging membrane. This technique works nicely to cut these membranes and also allows me to aspirate blood without having to switch to another instrument.
Dr. Heier: I have started to appreciate the increased safety. When we started using small-gauge cutters, I was doing more cases, and I could tell that working peripherally, it was much easier work in the presence of bullous retina. When operating on patients with diabetes, especially those with severe proliferative disease, I could use the cutter more as a tool rather than just a cutter. As the fellows started to take over, however, I really saw how much safer it was. They had to get much closer to the tissues and be right up against the pathology before any movement occurred. If they were shaving peripherally and not getting right into the vitreous that we wanted them to shave, there was very little movement of the retina and the vitreous. It showed me how much safer the cutters were.
Dr. Awh: Do your fellows find it natural to back off the vacuum rate to achieve very low rates of flow at high cut rates?
Dr. Heier: Yes, absolutely. What was interesting was, as experienced surgeons, we would see the area that needed to be shaved, and we would see the thin rims of vitreous, and we would intuitively go right up to that and shave that area with retina underneath. Fellows are taught to keep some distance from the retina, to stay away from those tissues and have the tissues or the vitreous come to them. With the increased efficiency of the cutters, I have found that when they get to those areas, especially with taut vitreous, they need to take the cutter right there. When they are there, they are cutting the vitreous, but they are still not getting movement of the retina.
|
"The longer cannula is an advantage because the longer the wound construction, the better the integrity of the wound at the end of surgery. This is one of the secrets of successful surgery." —Stanislao Rizzo, MD |
Dr. Awh: I have been impressed with how stable the detached retina is. Much of the information companies provide about cutter flow emphasizes maximum flow. If you look at the graphs in "Rewriting the Rules", which show vitreous flow rates of the MVE cutter vs the Alcon cutter, you see that at 2500 cpm, the Alcon cutter is capable of hardly any flow at all — almost zero — while the MVE cutter is capable of quite high flow. It is important for surgeons to realize that this does not mean the MVE cutter has only high flow at these high cut rates. Simply by changing the aspiration levels, we can go from zero to that maximum flow rate. My observation has been that with very low rates of vacuum and a high cut rate, we can perform safe and controlled removal of vitreous near the surface of the retina.
Dr. Chow, when fellows finish your program, enter practice and gain some experience, what method do you expect that they will use?
Dr. Chow: Most of us on this panel are comfortable using a cutter as a multipurpose tool and taking advantage of high speed and low flow to create a situation where we can do diabetic dissections quickly and well. For less-experienced surgeons, however, a typical diabetic dissection can take up to 3 hours. Not that this is about speed, but there is no question that experience makes a huge difference. I think most surgeons learn you can use a high-speed cutter to deal with this type of pathology and do it well and efficiently.

|
"I have reduced my use of scissors by using the smaller-gauge vitrector. It is a nice advantage. The less you introduce instruments into and out of the eye, the less likely you are to have peripheral tears." —Kevin J. Blinder, MD |
Dr. Awh: That is a great point because many of our colleagues did not have their training or obtain the bulk of their experience with vitreous cutters that function in this manner. When surgeons get an opportunity to use new cutter technology, I predict most will quickly begin reducing their instrument exchanges and using their cutter more as a multipurpose instrument.
Dr. Blinder, you are in a large group practice. Have you seen an evolution in how your partners operate with this newer generation of high-speed cutters?
Dr. Blinder: More and more, we are doing less dissection with scissors and more with the cutters. This applies to the attending physicians (my partners) as well as the fellows. It is sometimes difficult to watch the fellows operate, but it is comforting to observe them perform a vitreous base dissection in the area of a detachment and know they are less likely to cause a hole in the detached retina with the newer, more efficient, high-speed cutters. The fellows evolve into whatever methods work best for them, which is the cutter, once they finish their training.
Dr. Awh: Some years ago, when we were beginning to look at better ways of removing vitreous with these cutters, someone commented that removing vitreous was not the real challenge. That may be true, but that does not recognize all the other things we can do with a vitreous cutter. So it is not simply removing the central vitreous, which we now can do at very high cut rates with high flow, but being able to work close to the retina safely, to reduce the need for other tools and to minimize our instrument exchanges.
FUTURE DEVELOPMENTS
Dr. Heier: In a recent issue of Retina, Humayun and colleagues from Eye Concepts Lab reported on port geometry and its influence on vitrectomy.4 The work they are doing is changing the science of cutter tips. For example, they have a grater-cutter tip that has 10 small holes placed together, which may enable us to work close to the retina with even greater safety. They have horizontal and vertical slits that are ideal for working on membranes or shaving the vitreous base. Because of the numerous advances we have seen in the past couple of years, I realize that we probably have much further to go, and future advances will continue to improve our outcomes.
Dr. Awh: That is a great point. As you know, Eye Concepts is a valuable partner for B&L in the development and evaluation of this technology. And it is true, we always think we have reached the pinnacle of what can be done, but there are many exciting things destined for the future of vitreous cutter technology. RP
| REFERENCES |
|---|
|