







Principles of Laser-tissue Interaction
The PASCAL Method of photocoagulation achieves therapeutic effects with shorter pulse duration, introducing a host of benefits.

BY PAOLO LANZETTA, MD
The basic principles of laser-tissue interaction in the eye are relatively well known to us as retinal specialists, and not much has changed in this area since the days of ruby and xenon lasers — until now. For the first time in many years, we have something different, the PASCAL Photocoagulator. In this article, I will review key points about laser-tissue interaction and share what we have learned in our practice about choosing effective PASCAL laser parameters.
The biophysics of laser-tissue interaction are fairly simple with regard to histopathology. It is somewhat more complicated to discuss the biochemical changes induced by laser photocoagulation, especially subthreshold, but I will review basic histopathologic concepts here.
The real target when we are treating the retina is the retinal pigment epithelium (RPE) layer. Light is transformed into heat at the RPE cells, and temperature increases. Once the temperature has increased, heat spreads into the surrounding tissue, both vertically and laterally, widening the area of damage in the cells and tissue. With traditional photocoagulation, damage occurs not only in the RPE cells but also in the inner layers of the retina. This produces the so-called desired endpoint, which is the retinal whitening that corresponds to the therapeutic effect.
We have evidence that use of the PASCAL Photocoagulator can induce less damage, less whitening or even no whitening at all, and still achieve a therapeutic effect. Again, our goal is to target the RPE alone. We do not want cell and tissue damage to extend to the inner retina.
LASER PARAMETERS THAT INFLUENCE TREATMENT
Several factors influence the effects of laser photocoagulation treatment. The most important is wavelength. This is not because one wavelength is more effective than the other but because different wavelengths are absorbed to a greater or lesser extent by the target RPE cells. The green wavelength is absorbed quite well by the RPE cells and the choroidal melanin, which makes treatment relatively easy for the physician. This is why the 532-nm wavelength is so commonly accepted.
Another important factor is power. When the power is increased so is the damage caused. The third crucial factor that influences the effects of laser photocoagulation is pulse duration, or exposure time. In general, longer pulse duration causes more damage. Therefore, if pulse duration can be reduced, the unnecessary damage can be reduced as well.
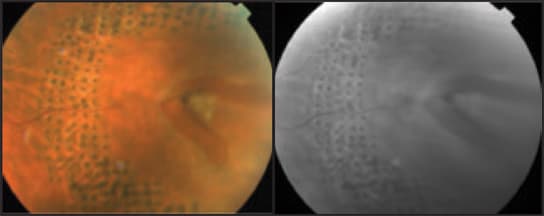
Figure 1. Color and red free photographs demonstrate the improvement in a peripheral retinal break 1 month after treatment with PASCAL laser irradiation.
This brings us to the PASCAL Photocoagulator. It delivers short pulses, in the range of 10-20 milliseconds, which may confine thermal damage to the outer retina. The decrease in exposure time compared with conventional treatment, which typically pulses at 100-200 milliseconds, means we can use less energy per pulse.
Short exposure time is not the only unique aspect of the PASCAL system. The system also allows us to place different shaped patterns onto the treatment area. In addition to choosing the shape, we can choose the dimension of the spots and the spacing between spots. Choosing a spot size of 400 μm (at the retina), for example, produces retinal whitening of 400 μm because the thermal spread is confined. A major enlargement of the spot does not occur at the retinal level.
The technology behind the PASCAL Photocoagulator clearly offers advantages over conventional retinal laser therapy. The shorter pulse duration and lower energy make the procedure less painful for patients. The physician has more control because he can choose spot size and ensure that spots are evenly spaced. In other words, treatments are more precise. They are also more efficient, due to the rapid delivery of the laser pulses. In the future, we also may find this technology to be the ideal way to treat patients while inducing no whitening at all at the retinal level.
EFFECTIVENESS WITH A GENTLER PROCEDURE
Over the past 2 years, we have performed more than 1000 procedures, in approximately 700 eyes, using the PASCAL Photocoagulator. Most of these cases have been proliferative diabetic retinopathy (PDR). We also have used PASCAL to treat diabetic macular edema (DME) as well as peripheral retinal holes and tears.
When we first began using the PASCAL Method of photocoagulation, we needed to gain some experience choosing the proper parameters for utilizing the shorter laser pulses. Once we worked that out, we were able to obtain the same results — regression of new vessels, reabsorption of macular edema, and so on — as we expect when treating with a traditional photocoagulator. However, with the PASCAL system, we are able to do so in a more precise and efficient manner.
For treating PDR, I typically use a power of 800-1200 mW and a 200-μm spot size with a quadraspheric lens (400 μm at the retina). In treatment-naïve patients, I generally use the 5 × 5 pattern array, which is a dense treatment, with 0.25 spot diameter spacing between spots. In most patients, I have been able to deliver a large number of spots in one session.
For treating DME, I use a power setting of 150-300 mW. I typically use the 60-μm spot size, which is very useful if I am using a quadraspheric lens (120 μm at the retina) for treating the posterior pole. I often use the single spot, most frequently with a 10-millisecond pulse duration. I occasionally use the 2 × 2 pattern array.
Reaching the retinal periphery is easy with the PASCAL Photocoagulator, which is not necessarily the case with all of the conventional lasers available today. Not much distortion of the laser spots occurs in the peripheral retina, even when a 5 × 5 pattern or 3 × 3 pattern array is used. The typical power for peripheral treatments is 300-700 mW. I often use a spot size of 200 μm (at the slit lamp) and either the 3 × 3 or 2 × 2 pattern array to make a nice contour around the lesions.
It is important to note that the ideal power setting will vary from patient to patient, based on the variation in pigmentation. Even in the same patient, if areas with major differences in fundus pigmentation are present, the power should be adapted accordingly.
TAKING PHOTOCOAGULATION TO THE NEXT LEVEL
In our practice, the PASCAL Photocoagulator has taken the "boredom" out of performing laser treatments. More importantly, this technology gives us the opportunity to provide less invasive, less time-consuming and less painful care for our patients. It provides an elegant foundation for combination therapy involving vascular endothelial growth factor inhibitors or steroids. Other interesting future directions, such as subthreshold treatments, are being explored. I expect the PASCAL Method to play an increasingly important role in the treatment of patients with diabetic eye disease as it is used in combination with steroids, anti-VEGF drugs and other new medications. RP
Paolo Lanzetta, MD, is an associate professor in the department of ophthalmology at the University of Udine in Udine, Italy.