







Management of the Diabetic Patient
The "laser plus" approach incorporates the latest in imaging, pharmacotherapy and photocoagulation for the best possible outcomes.

BY ADRIAN KOH, MD
The approach I take to managing patients with diabetes has evolved over the past few years, as it has for many retinal specialists around the world. While we still consider laser photocoagulation to be the gold standard for the treatment of diabetic retinopathy in our practice, our efforts have benefited from the adoption of spectral domain optical coherence tomography (OCT), the PASCAL Method of photocoagulation and pharmacologic treatment options.
OCT PLAYS AN INCREASINGLY IMPORTANT ROLE
We are all familiar with the images obtained first with the Stratus OCT (Carl Zeiss Meditec, Dublin, Calif.) and more recently with spectral domain OCT devices. Beyond their utility in timing repeat injections of anti-vascular endothelial growth factor (VEGF) agents, the spectral domain images provide previously unavailable information that is similar to optical biopsies. I have found them useful in guiding decision-making in several scenarios. For example, when retinal thickening is sponge-like, I expect it to respond adequately to focal grid laser treatment, and I can typically withhold adjuvant therapy. However, when I see cystic spaces or degeneration and a large volume of subretinal fluid, which usually signals significant ischemia or perhaps long-standing changes, I consider it necessary to employ adjuvant therapy. In addition, OCT provides the ability to differentiate vitreoretinal interface problems that may require vitrectomy rather than medical management.
In some cases, OCT is useful as a prognostic tool. For example, reflectivity from inner retinal layers can serve as an objective criterion for predicting visual outcomes following intravitreal injection of triamcinolone acetonide (IVTA). A thick hyper-reflective inner layer often indicates a better prognosis. A thin, hyporeflective inner layer often indicates a poorer prognosis, which should be discussed with the patient. I have also used OCT to map and plan focal and confluent laser photocoagulation around the macula, which is simple and quite effective.
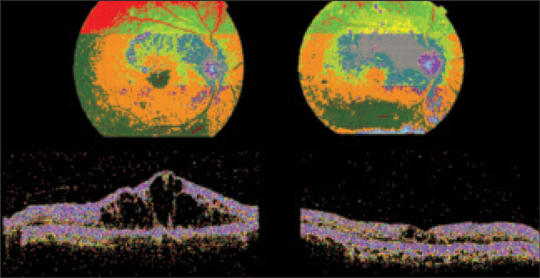
Figure 1. The images on the left show the patient's OCT pretreatment, with visual acuity 6/60. The images on the right show the patient 1 month after treatment with intravitreal triamcinolone. Visual acuity has improved to 6/12.
LASER THERAPY CONTINUES TO BE FUNDAMENTAL
In addition to OCT, laser photocoagulation is a staple in my practice. I believe it continues to be fundamental to the effective management of diabetic retinopathy. We have solid evidence of its benefits from several well-designed randomized controlled trials. It has been proven to prevent vision loss in proliferative diabetic retinopathy (PDR) and in clinically significant macular edema (CSME). It has been proven to increase the chances of vision improvement in CSME. Perhaps its chief benefit, even in the age of anti-VEGF therapy, is the long-term stability and durability of action.
However, we are aware of the disadvantages of laser therapy as well. It does take time for the effects to appear, sometimes as long as 4-6 weeks. Initially it may aggravate edema and perhaps worsen vision, which tends to make patients lose confidence. Vision often remains poor in severe cases, especially diffuse cystoid macular edema (CME), and conventional pan-retinal photocoagulation (PRP) is known to worsen CME. There are known potential side effects as well, such as reduced accommodation, visual field defects, night vision disturbance, PRP scar enlargement and iatrogenic choroidal neovascularization.
The PASCAL Method of photocoagulation, due to its gentler burns of shorter duration, has minimized many of these side effects in my patients. Conventional photocoagulation heats a large volume of tissue, causes collateral damage and inflammation, damages the retinal nerve fiber layer and affects the pain receptors located in the choroid.
In contrast, the PASCAL Method transfers less heat to the choroid, which improves patient tolerance. It also provides potential clinical benefits consequent to reduced inflammatory response and preservation of the retinal nerve fiber layer.1,2
JUDICIOUSLY APPLIED, COMBINATION THERAPY PROVIDES ADVANTAGES
I consider my current approach to diabetic retinopathy to be "laser plus" therapy — laser plus something else — in other words, combination therapy. The combination may include posterior sub-Tenon's triamcinolone, IVTA or any of the anti-VEGF agents. Adjunctive intravitreal therapy provides several benefits, including rapid onset of action, especially with the anti-VEGF agents, and dramatic visual improvement. Patients are usually quite satisfied. Adding intravitreal therapy also eliminates the initial worsening of vision that might be caused by the initiation of laser therapy. It is effective in cases involving media opacities; it controls neovascularization and, as a pretreatment, may potentially make macular laser safer. At the same time, the disadvantages of intravitreal therapy must be considered. It is invasive and can be potentially blinding with a complication such as endophthalmitis, which is especially relevant in diabetic patients. The effects may be short-lived. Furthermore, long-term treatment may impair neuroprotection. The high recurrent cost of treatment is also an issue.
IVTA was originally used to treat cases of diffuse diabetic macular edema (DME), which respond quite well to this approach. The treatment effect often persists for at least 3 months and sometimes up to 6 months. Problems with IVTA of course include increased intraocular pressure and significant cataract. Sub-Tenon's administration has been attempted in an effort to reduce these side effects. Unfortunately, although the pressure was lower, the treatment effects were not as dramatic or long-lasting as IVTA.3
Interestingly, studies have shown that combining laser treatment with IVTA produces a more durable effect than IVTA alone.4 This serves to highlight a key aspect of current care, which is that laser remains fundamental to any form of combination therapy for diabetic eye disease.
We also have biological and scientific rationale for using anti-VEGF agents in the treatment of diabetic eye disease — DME in particular. Numerous studies have shown that VEGF is overexpressed in various forms of the disease. Numerous ongoing and published studies indicate that anti-VEGF agents are safe and clinically effective in terms of both improved visual acuity and reduction of macular thickness on OCT.5-7 However, although the effects are dramatic while patients are on treatment, edema tends to return when treatment is suspended. Furthermore, the effects of long-term VEGF blockade are unknown. Might it decrease neuroprotection, impair retinal/choroidal perfusion or exacerbate macular ischemia? Potential adverse systemic effects in already high-risk patients are a concern as well.
Also of note, some studies have suggested bevacizumab (Avastin, Genentech) may be inferior to triamcinolone in the treatment of DME over the long-term.8
CASES REPRESENTATIVE OF THE ‘LASER PLUS’ TREATMENT APPROACH
Two of my cases clearly illustrate the expected outcomes when we utilize all of the treatment tools at our disposal, including a combination approach. The first case involves a 48-year-old male with poorly controlled Type 2 diabetes (11.2% HbA1c). He experienced progressive blurring of vision in both eyes and had previously undergone bilateral grid and very light scatter laser treatment at another practice. When he presented at our practice, his visual acuities were 6/24 OD and 6/60 OS. Rubeosis was not present, but we found significant bilateral cataracts. Gross edema (566 μm) was present OD. Fluorescein angiography showed PDR and diffuse CME. In the left eye, there were no new vessels, but we noted widespread ischemia and diffuse CSME.
Consistent with my treatment approach, I administered intravitreal ranibizumab (Lucentis, Genentech) and PRP with the PASCAL Photocoagulator bilaterally. The response in the right eye was dramatic. Within 1 week, retinal fluid regressed and vision improved to 6/12. By 3 weeks after the injection, visual acuity improved even further, to 6/9 despite the cataract. However, just as the effect of the ranibizumab began to wear off, macular thickness began to climb.
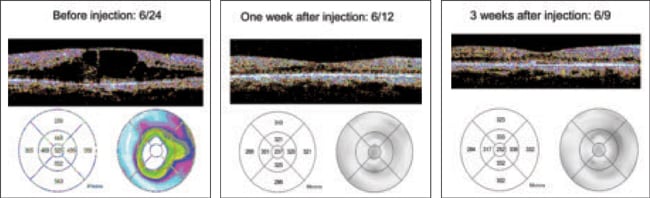
Figure 2. A patient treated with ranibizumab (Lucentis, Genentech) showed remarkable improvement after just 1 week. However, just as the effect of the ranibizumab began to wear off, macular thickness began to climb.
Results of initial treatment were similar for the left eye. Two weeks after injection, acuity improved to 6/7.5, and marked restoration of the foveal architecture and drying of the macula occurred. By 4 weeks post-injection, visual acuity decreased and edema returned. This patient therefore required more injections and more PRP in the left eye.
Each eye received 3 monthly doses of ranibizumab and 4 additional sessions of PRP. The patient then underwent bilateral uneventful phacoemulsification surgery, after which, as expected, the DME returned and further ranibizumab injections were needed. The right eye received 4 injections and the left eye received 6 injections. However, 1 year later, both eyes are doing well. The patient has not received an anti-VEGF injection in 6 months.
A second case involves a 49-year-old male with obesity, good glycemic control (6.9% HbA1c), hypertension, dyslipidemia and bilateral diffuse CME. This patient also has a family history of blindness due to diabetic retinopathy. The referring ophthalmologist had treated with bilateral PRP, but vision in both eyes was deteriorating, to counting fingers OD and 6/60 OS.
In this case, starting with the right eye, I administered PASCAL Method PRP and ranibizumab. One day after initial treatment the macular edema improved slightly and there was no aggravation of the CME despite placing 1500 laser burns in the eye. As time passed, this patient also required intravitreal steroid treatment with dexamethasone to control the edema. Two weeks after the steroid was added to the laser and ranibizumab treatments, the edema was almost completely resolved. Small pockets of cystic spaces remained, but visual acuity had improved to 6/12. Similar treatment was carried out for the left eye, with good results.
PATIENCE, PERSISTENCE NEEDED TO ACHIEVE POSITIVE OUTCOMES
In summary, OCT has become an invaluable tool for assessment and therapeutic decision-making for my diabetic patients. PASCAL PRP and focal and grid lasers remain the foundation of good and long-lasting control of diabetic retinopathy. I have found that adjunctive intravitreal therapy, especially anti-VEGF agents, markedly improves outcomes, but that I have to expect repeat injections. Patience and persistence are necessary for reaching treatment goals. Finally, refractory cases of diabetic eye disease may require long-term IVTA treatment in addition to laser and anti-VEGF therapy, and cataract and increased intraocular pressure continue to be major obstacles. RP
Adrian Koh, MD, is founding partner and senior consultant at the Eye & Retina Surgeons, Camden Medical Centre, director of Retinal Centre International, and vice-president of the International Retinal Foundation, all in Singapore. He is also a visiting consultant to the Singapore National Eye Centre and visiting consultant to the Eye Institute, Tan Tock Seng Hospital.
| REFERENCES |
|---|
|