







Laser vs Pharmacotherapy for Diabetic Eye Disease
Why the answer is not one or the other.

BY GEORGE A. WILLIAMS, MD
As vitreoretinal specialists, we have clearly arrived at a transition period. We are now able to address a variety of posterior segment diseases not only with laser therapy or vitrectomy but also with pharmacologic agents. Therefore, of course, we would like to know which is the best approach. This question is about the art of translating clinical trials and basic science into clinical practice. Here, I present several points relevant to our consideration of pharmacologic therapy and laser photocoagulation for the treatment of diabetic macular edema (DME).
We all know that DME is a complex disease process characterized by the breakdown of the inner and outer blood-retinal barriers. This produces changes in microvascular permeability, which lead to extracellular edema, photoreceptor distortion and loss of vision. We also know that diabetes is a systemic disease. Therefore, we must be tuned into our patients' status as it relates to glycemic control, hypertension, renal function and lipids. We must be aware of the use of systemic drugs with the potential to aggravate macular edema, particularly with the widespread use of the glitazone medications, such as rosiglitazone (Avandia, GlaxoSmithKline).
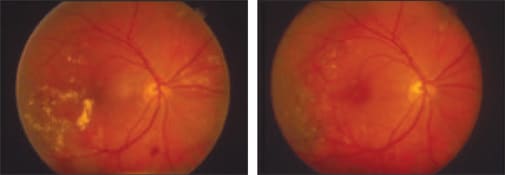
Figure 1. At left, a patient with clinically significant macular edema is shown pretreatment. The other image shows the same patient after laser treatment.
KEY CONSIDERATIONS: EFFICACY, SAFETY AND VALUE
To compare pharmacologic therapy with laser photocoagulation, we need to consider 3 primary areas: efficacy, safety and value.
There is little doubt that photocoagulation remains the standard for the treatment of DME. The best data and the best long-term clinical experience are available for this modality. The Early Treatment of Diabetic Retinopathy Study (ETDRS) demonstrated the visual benefits of focal photocoagulation. The published data from this study show a dramatic clinical effect. However, we also see that even with appropriate photocoagulation, 12% to 20% of patients will continue to have vision loss at 3 to 5 years. In addition, we see that focal disease responds well to laser, but diffuse disease, macular traction and macular ischemia respond poorly.
Even though we have been employing laser treatment for many years, we still do not fully understand its mechanism of action. It is most likely a combination of anatomic and biochemical events that change the hemodynamics of the retina.
We do have solid information regarding the best technique for laser photocoagulation. A variety of adjustments to the ETDRS technique have been suggested. The Diabetic Retinopathy Clinical Research Network recently conducted a comparison of 2 techniques for treating DME: the modified ETDRS direct/grid technique and a milder (but potentially more extensive) macular grid technique.1 In the latter, microaneurysms are not treated directly, and small mild burns are placed throughout the macula, whether or not edema is present. At 1 year, no difference in vision outcomes was observed, despite the fact that the ETDRS technique reduced macular edema more. Based on the results, the researchers concluded that modified ETDRS photocoagulation should continue to be the standard approach for treating DME.
Overall, the benefits of laser therapy are well established. The clinical effect is easily titrated; the effects are long-lasting. There is minimal ocular toxicity, no systemic concern, and it is cost-effective.
EXAMINING THE VALUE EQUATION
The advent of pharmacotherapy for DME has been driven by the elucidation of the condition's molecular mechanisms and the variable efficacy of laser in some patients. Weknow, because of our understanding of molecular mechanisms, that combinations of drugs can be effective because they target multiple mechanisms of action. We are all familiar with the rationale behind the use of steroids, vascular endothelial growth factor (VEGF) inhibitors and a relatively new class of drug, protein kinase C (PKC) inhibitors.
When using drugs to treat retinal disease, we have to be aware of potential complications. For example, we must consider whether there is a safety difference between ocular and systemic inhibition of VEGF. We have to consider how frequently treatment must be administered and for how long. We also need to consider short-term vs long-term effectiveness and safety. Finally, the cost and value of the treatment are key considerations.
When we look at treatment value, we can consider clinical endpoints. We must ask ourselves: What is the treatment's effect on the patient's quality of life? In other words, it is a question of statistical significance vs clinical relevance. One way to consider this concept is to look at the number needed to treat (NNT). The NNT is the inverse of the absolute risk reduction, which is the difference in rates of outcomes between experimental and control participants in a trial. NNT conveys both statistical and clinical significance, which is increasingly important in a drug-based treatment era.
Some examples of NNT calculations:
• ETDRS laser photocoagulation
In the ETDRS data, we find a 48% risk reduction for the endpoint of moderate vision loss. The probability of this endpoint was 23% with placebo and 12% with treatment, an absolute reduction of 11%. This results in an NNT of 9 [1/(23-12)], meaning the treatment would need to be applied to 9 patients for 1 patient to benefit.
• Ruboxistaurin for macular edema
Taking the same endpoint of moderate vision loss from the ruboxistaurin study data,2 we have a risk reduction of 40%, similar to the risk reduction for ETDRS laser photocoagulation. However, the absolute risk reduction, 9.1% for the placebo group minus 5.5% for the treatment group, is only 3.6%. In this case, the NNT is 28 [1/(9.1-5.5)]. In other words, 28 patients must be treated for 1 patient to benefit.
When considering NNT, it is not possible to accurately compare trials with different inclusion criteria. However, NNT is useful for determining the clinical relevance of respective treatments that have been studied with similar inclusion criteria and endpoints. When cost and safety are also taken into account, NNT helps to determine the value of a treatment.
MEDICINE: THE SCIENCE AND THE ART
A substantial amount of information about laser therapy and pharmacotherapy is available for us to consider when treating patients with diabetic eye disease. But in the absence of direct comparisons via randomized controlled clinical trials, we are without a clear-cut answer as to which is best.
However, the question is no longer whether we should be using laser or drugs. We know that complex diseases are rarely cured or controlled with monotherapy. And we now have improved photocoagulation technology, the PASCAL Method, which clearly minimizes the destructive effects associated with conventional laser therapy.
Therefore, we can begin to look at treatment paradigms that combine photocoagulation with other modalities. We must consider both the anatomical and molecular mechanisms of the disease process and apply what we know using a patient-specific approach that combines photocoagulation, drugs and even surgery in select patients. RP
George A. Williams, MD, is chairman of the department of ophthalmology and director of the Beaumont Eye Institute at William Beaumont Hospital in Royal Oak, Mich. He is also a clinical professor of Biomedical Sciences at the Eye Research Institute of Oakland University in Rochester, Mich. He is a member of the OptiMedica Medical Advisory Board.
| REFERENCES |
|---|
|