







PEER REVIEWED
Infectious Retinitis: A Review
YACHNA AHUJA, MD · STEVEN M. COUCH, MD · RAYMUND R. RAZONABLE, MD · SOPHIE J. BAKRI, MD
Infections of the retina are potentially devastating diseases because they can lead to permanent vision loss. Often, infectious retinitis is the initial clinical manifestation of a more systemic illness. Infectious retinitis affects both immune-competent and immune-compromised individuals. While seroepidemiologic studies reveal that certain pathogens such as cytomegalovirus (CMV) are ubiquitous in humans, retinitis caused by CMV is uncommon and is observed mainly in individuals with compromised cell-mediated immunity such as those with advanced AIDS. Likewise, retinitis caused by Toxoplasma gondii is seen more commonly in individuals with impaired immune function. On the other hand, certain infectious retinitis, such as that due to tuberculosis or syphilis, occur regardless of the immune status of the host, and in some cases, such as tuberculous retinitis, it is seen more commonly in endemic areas. Infectious retinitis requires early and aggressive treatment in order to avoid its potentially blinding outcome. The type of treatment relies on pathogen identification, and, in many cases, systemic administration of anti-infective therapy is required in view of underlying systemic infectious disease syndrome and to prevent the involvement of the contralateral eye. This article reviews a selected list of the more common endogenous infections affecting the retina with the aim of discussing disease pathogenesis, clinical presentation, diagnosis, and treatment.
| Yachna Ahuja, MD, and Steven M. Couch, MD, are residents in the Department of Ophthalmology at the Mayo Clinic in Rochester, MN. Raymund R. Razonable, MD, is associate professor of infectious disease at the Mayo Clinic. Sophie J. Bakri, MD, is assistant professor of ophthalmology at the Mayo Clinic. The authors report no financial interest in any products mentioned in this article. Dr. Bakri may be reached via e-mail at bakri.sophie@mayo.edu. |
CYTOMEGALOVIRUS RETINITIS
Cytomegalovirus, an enveloped double-stranded DNA virus belonging to the Herpesviridae family, is a common human infection with estimated seroprevalence rates reaching 90% to 100% in some populations. Several modes of transmission occur, including in utero (congential infection) and through urine, saliva, breast milk, sexually transmitted fluids, organ transplantation, and blood transfusion. Primary CMV infection universally leads to a latent state in many cells, which serve as reservoirs for transmission and reactivation during periods of immunodeficiency. Acute CMV infection during pregnancy can lead to congenital infection of the immunologically immature fetus, and up to one-quarter of infants with symptomatic congenital CMV infection manifest with retinitis.1,2 Reactivation of latent CMV in immunosuppressed individuals, such as those with AIDS (when CD4+ T cell count is <50 cell/mm3) or organ and stem-cell transplant recipients, leads to disseminated disease involving several organs, including the retina.3
However, during the past 10 years, with earlier detection of human immunodeficiency virus infection and initiation of highly active antiretroviral therapy (HAART), CMV retinitis is becoming less commonly seen in patients with AIDS. Compared to patients with AIDS, CMV retinitis is less commonly seen in recipients of organ and stem-cell transplantation.6
Cytomegalovirus causes full-thickness retinal necrosis with pathognomonic cytomegalic cells with intranuclear inclusions.7 Clinically, CMV retinitis presents with blurred vision and floaters, especially in those with lesions in the posterior pole. CMV papillitis, which affects less than 10% of eyes, may present with sudden loss of vision.8,9 Examination generally reveals 1 to 2 lesions in each eye that can be adjacent to blood vessels and in 1 or more of 3 zones.10 Zone 1 lesions are 1 to 2 disc diameters from the fovea and the optic nerve, and they are associated with sudden reductions in visual acuity (VA). Zone 2 lesions are located up to the vortex veins, with zone 3 extending from zone 2 to the ora serrata. Zone 3 lesions are highly associated with retinal detachments.11,12 The hallmark CMV lesion is white with irregular granular borders, associated hemorrhage, and small "satellites" at the advancing edge (Figure 1). The associated vitritis and anterior uveitis are usually mild. There are 2 distinct variants of CMV retinitis.13 "Fulminant" lesions have marked edema with confluent areas of retinal whitening, retinal hemorrhage, and vascular sheathing. "Indolent" lesions are round granular lesions in the peripheral retina, with little associated edema and faint opacification.14 Untreated CMV lesions usually enlarge rapidly, with the entire retina being destroyed within 6 months or less, especially in individuals with persistent immune compromise.15
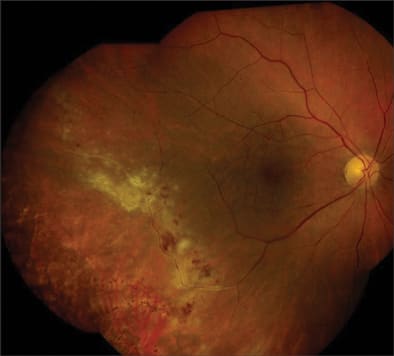
Figure 1. Classic CMV retinitis extending along inferotemporal arcade. Note the white area of inflammation with associated hemorrhage and satellite lesions at advancing border.
The diagnosis of CMV retinitis is primarily based on clinical grounds, although CMV detection by polymerase chain reaction (PCR) of aqueous and vitreous humor can be done for atypical cases.16,17 In some cases, CMV may be detected in blood and other body fluids, although in many cases, CMV retinitis is compartmentalized. Treatment of CMV retinitis involves an induction phase, with high doses of anti-CMV agents, followed by a maintenance phase, which is aimed at both halting the progression and preventing the recurrence of disease. The most common agent used is intravenous (IV) ganciclovir (Cytovene, Roche) or its oral alternative, valganciclovir (Valcyte, Roche). Ganciclovir can also be given through intravitreous route, as an injection or an implant (Vitrasert, Bausch & Lomb, Rochester, NY). Oral ganciclovir should not be used for treatment since it is poorly absorbed and has low bioavailability. Other alternative drugs are IV foscarnet (Foscavir, AstroZeneca) and cidofovir (Vistide, Gilead Sciences, Foster City, CA). All 3 drugs are virostatic and halt CMV replication by inhibiting CMV DNA polymerase. In contrast, a fourth anti-CMV drug, fomivirsen (Vitravene, Isis Pharmaceuticals, Carlsbad, CA), acts through an antisense mechanism.18
The most common initial treatment course for CMV retinitis in patients with AIDS includes IV ganciclovir at a dose of 5 mg/kg twice daily for 3 weeks, followed by maintenance therapy with either IV ganciclovir or oral valganciclovir. At a dose of 900 mg orally per day, valganciclovir achieves similar serum concentrations as IV ganciclovir 5 mg/kg,19 and, hence, valganciclovir, at a dose of 900 mg twice daily for 3 weeks, has been shown to be equally effective and comparable to IV ganciclovir for induction treatment of CMV retinitis in patients with AIDS. The use of the ganciclovir implant has led to a much longer median time to progression of CMV retinitis compared to IV ganciclovir.20,21 Though ganciclovir is associated with bone marrow suppression, systemic administration of ganciclovir is highly recommended — even in patients treated with the ganciclovir implant since CMV disease is often a disseminated illness — to prevent the involvement of the contralateral eye. The use of IV foscarnet is limited by side effects of electrolyte disturbance and nephrotoxicity.22 Intravenous cidofovir has a long half-life, enabling its once weekly dosing.23 However, cidofovir is highly nephrotoxic and is associated with sight-threatening uveitis and hypotony; hence, it is less commonly used. Clinical trials with fomivirsen have shown that it is effective for CMV-retinitis refractory to other drugs, and it also increases the time to disease progression.24,25 Drug resistance can develop during treatment with each of these agents, particularly in patients with persistent immune compromise and with the use of poorly bioavailable agents such as oral ganciclovir.26,27
The most common complication of CMV retinitis is retinal detachment. In AIDS patients with CMV retinitis, it is important to start HAART therapy, although immune recovery uveitis can develop with its initiation,28-30 and this can lead to severe vision loss and may require treatment with anti-inflammatory agents.
ACUTE RETINAL NECROSIS AND PROGRESSIVE OUTER RETINAL NECROSIS SYNDROMES
Varicella zoster virus (VZV) and herpes simplex virus (HSV) types 1 and 2 have been implicated as the etiologic agents of progressive necrotizing retinopathies including acute retinal necrosis (ARN), which is classically described in immunocompetent patients, and progressive outer retinal necrosis (PORN) syndrome, which is seen in immunocompromised patients.
Acute retinal necrosis, which may involve one or both eyes of healthy patients (and less commonly, in immunocompromised patients)31-33 is characterized by anterior uveitis, vitritis, and retinal vasculitis with patchy or confluent areas of cream-colored retinal necrosis (Figure 2) that initially affects the peripheral retina and then extends posteriorly, often leading to retinal detachment.34-37 The diagnosis of ARN is based on clinical grounds and supported by demonstration of the offending herpes virus with techniques such as PCR of intraocular specimens.38-40 In contrast, PORN is seen in immunocompromised patients with a paucity of uveal inflammation and vasculitis, characterized mainly by outer retinal discoloration in the posterior pole, which spreads rapidly throughout the fundus.41
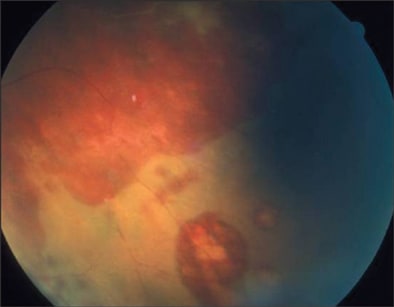
Figure 2. Acute retinal necrosis, showing an advancing border of necrosis with atrophic areas and holes.
Although there are limited reports of successful combination antiviral treatment for PORN with acyclovir, foscarnet, and ganciclovir, PORN usually shows rapid progression and carries a very poor prognosis.42,43 The management of ARN varies, depending on the severity of disease.44 Antiviral treatment should be given promptly, with either IV acyclovir, oral valaciclovir, or famciclovir (Famvir, Schering-Plough).45-47 A common treatment strategy is IV acyclovir 1500 mg/m2, divided every 8 hours for 7 days followed by 4 to 6 weeks of oral acyclovir, 2 to 4 g/day.44 Systemic and topical corticosteroids are often added to minimize the inflammatory damage to the optic nerve and blood vessels.48 Since many severe cases also involve an occlusive vasculitis, low-dose aspirin is added as antithrombotic treatment.49,50 Surgery may be needed to repair rhegmatogenous retinal detachments. Prophylactic argon laser treatment has been used to reduce the risk of this complication, although its use is controversial in the treatment of ARN. The visual prognosis of ARN is poor, particularly in cases caused by VZV.51-54
ENDOGENOUS FUNGAL INFECTIONS OF THE RETINA
Fungal infections of the retina are among the most devastating ocular infections.55 Two types occur according to mode of acquisition. Endogenous fungal retinitis occurs as a component of disseminated fungal diseases, while exogenous fungal retinitis occurs after ocular trauma or surgery. The most common among these infections is candidal chorioretinitis, usually caused by Candida albicans, although other species of candida have also been observed.56 Factors that could predispose to candidemia and candidal chorioretinitis include recent major surgery, bacterial sepsis, indwelling intravenous catheters,57-60 and intravenous drug abuse.61,62 Candidal retinitis is also the most common intraocular fungal infection of newborns.63,64 Endogenous candidal chorioretinitis usually presents with decreased vision, as well as pain due to associated anterior uveitis or iridocyclitis. The vitreous is typically hazy, overlying a white circumscribed lesion of less than 1 mm in diameter (Figure 3). Diagnosis is usually clinical, although the vitreous humor can be cultured.65
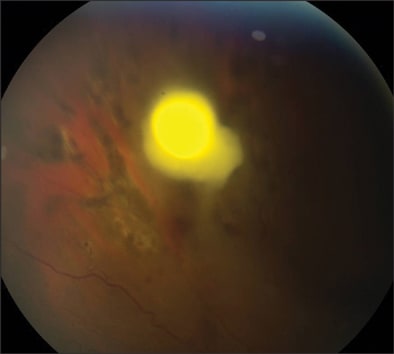
Figure 3. Candidal endophthalmitis. Vitreous inflammation obscures some details of the photograph; however, the dense fluffy localized infiltrate is characteristic.
Aspergillus species is the second most common fungal group that infects the choroid and retina. Aspergillus fumigatus retinitis is seen mostly among intravenous drug abusers, patients who have received transplants, and those with malignancy and chronic lung diseases.66-69 The lesions are characterized as yellow subretinal and retinal infiltrates in one or both eyes, associated with rapid vision loss, severe inflammation, and retinal hemorrhage.70 Aspergillus species is a highly vasculotrophic fungus. Retinal vessels can be invaded, resulting in thrombosis, infarction, and retinal necrosis.71 In severe disease, septate branching hyphae can be found throughout the eye. This is usually associated with disseminated disease and pulmonary involvement. Serologic tests are not helpful and cultures of the blood are often negative.72
Cryptococcus neoformans is a common cause of intraocular fungal infection in AIDS patients.73-75 Ocular involvement is frequently associated with cryptococcal meningitis, although retinal lesions may also be present without or prior to the onset of meningitis.76,77 Initial symptoms are intermittent blurring of vision that can progress to severe endophthalmitis with associated meningeal or systemic infection.78,79 Multifocal chorioretinitis is the most common finding with yellowish-white fundus lesions of various sizes and associated mutton-fat keratic precipitates, exudative vitreous detachment, and vitritis.80,81
The prevalence of intraocular fungal infections may have decreased over the past decade due to availability of well-tolerated antifungal agents for prophylaxis in immunocompromised patients, the early initiation of systemic antifungal therapy based on positive blood cultures, and the recovery of immune function in patients with AIDS who are receiving HAART.82,83 When it occurs, however, fungal ocular infection should always be treated, since failure to treat usually results in severe endophthalmitis and vision loss.84 The drugs that may be used for the treatment should be guided by the specific fungal pathogen. While conventional and lipid formulations of amphotericin B have traditionally been considered as the drugs of first line, their use is limited by systemic toxicities, including renal failure and anaphylaxis.85 Flucytosine is sometimes combined with amphotericin B to facilitate fungal clearance, although flucytosine should never be used alone because of the rapid development of drug resistance.86
The azole class of antifungal drugs offers a well-tolerated regimen for the treatment of many fungal infections. Fluconazole (Diflucan, Pfizer) is effective as treatment for C. albicans retinitis or as a "step-down" treatment after initial treatment with amphotericin B, although other studies have noted treatment failure.87-90 Newer triazoles such as voriconazole (VFEND, Pfizer) and posaconazole (Noxafil, Schering-Plough) have supplanted amphotericin B for the treatment of invasive aspergillosis. Voriconazole has been demonstrated to have good ocular penetration, and thus it has been reported as useful for the treatment of fungal retinitis.91-93 The echinocandins, such as caspofungin (Cancidas, Merck), micafungin (Mycamine, Astellas), and anidulafungin (Eraxis, Pfizer), are highly active against Candida species and Aspergillus species (but not C. neoformans); however, poor penetration into the ocular compartments is a concern and their utility for the treatment of fungal retinitis is therefore questionable. Due to the common association with systemic disease, the intravenous and oral route is generally used for the administration of antifungals in the treatment of endogenous fungal endophthalmitis; however intraocular antifungal therapy with agents such as amphotericin B and voriconazole also has an important adjunctive role.94 Vitrectomy is a useful adjunct therapy if there is severe vitreous involvement or failure of medical therapy.95.96
OCULAR TOXOPLASMOSIS
Ocular toxoplasmosis is a potentially blinding retinitis caused by the obligate intracellular parasite T. gondii. Felines are the definitive hosts of the parasite, but it can be transmitted to humans through contaminated meat and eggs.97,98 T. gondii can persist as latent infection in humans for many years by living within host-cell vacuoles (tissue cysts) in any organ. In immunocompromised hosts, the cyst ruptures and leads to dissemination of T. gondii to cause systemic illness that includes panophthalmitis and retinitis.99
Within the eye, tissue cyst rupture can cause an active focal necrotizing retinitis followed by scar formation.100 This may be directly due to parasitic proliferation, while overlying effects such as vitritis and anterior uveitis may be due to a hypersensitivity response.101 Active lesions are identified as localized areas of infiltrate (Figure 4). Classically, these active lesions are adjacent to old inactive scars and focal vasculitis. The 3 morphological variants of these lesions are large destructive lesions, punctate inner retinal lesions, and punctate outer retinal lesions.102 Secondary complications, such as cataract, glaucoma, cystoid macular edema, and chorioretinal vascular anastomoses, can occur. A minority of patients may have toxoplasmic papillitis, where the foci of inflammation are adjacent to the optic nerve head.103
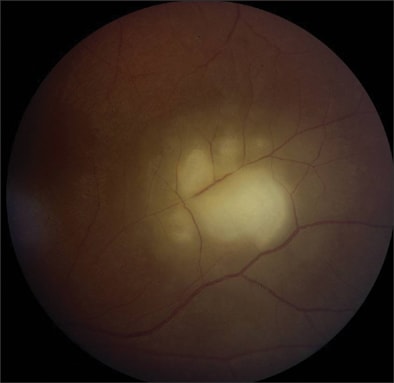
Figure 4. Toxoplasma gondii retinochoroiditis. Notice the well-circumscribed area of retinochoroidal edema.
Symptoms of ocular toxoplasmosis include floaters or reduced vision. In children with congenital toxoplasmosis, initial signs include nystagmus or strabismus, with over 80% developing retinochoroiditis by adolescence. Of these cases, up to 40% are bilateral.104 The diagnosis of ocular toxoplasmosis is based on characteristic retinal scars, supported by serologic antibody tests such as the indirect fluorescent antibody test and the enzyme-linked immunosorbent assay (ELISA) tests. Definitive diagnosis is difficult since there is high prevalence of antibodies in healthy adults, although the presence of immunoglobulin M antibodies would indicate acute infection.105
The decision to treat ocular toxoplasmosis is based on the location of lesions, the extent of secondary effects, and the immune status of the human host. Large destructive lesions and posterior-pole lesions are associated with severe vision loss and are treated. Lesions that are small and peripheral may heal without treatment. Immunocompromised patients may require treatment regardless of the extent of the lesion at diagnosis. The most common treatment regimen includes the combination of pyrimethamine (Daraprim, GlaxoSmithKline) and sulfadiazine, and often corticosteroids are added.106 The addition of folinic acid to this regimen prevents leucopenia and thrombocytopenia due to pyrimethamine treatment. Therapy with trimethoprim-sulfamethoxazole or pyrimethamine-azithromycin has been shown to have equal efficacy and is considered an acceptable regimen for the treatment of ocular toxoplasmosis.107,108 Prophylactic pyrimethamine-sulfamethoxazole may be useful for recurrent attacks of ocular toxoplasmosis or after cataract extraction when there is a potential risk of reactivation.109,110 The use of prophylactic trimethoprim-sulfamethoxazole has reduced the incidence of toxoplasmosis after transplantation. The overall prognosis is usually good in immunocompetent individuals, as long as the central macula is not involved.111
OCULAR TOXOCARIASIS
Ocular toxocariasis is a common diagnosis in asymptomatic children and it is a major worldwide cause of vision loss.112-114 The roundworm Toxocara canis is transmitted by ingestion of fertilized ova, followed by systemic dissemination via the circulatory system. Systemic toxocariasis can range from mild eosinophilia to fatal disease involving pneumonia, congestive heart failure, or convulsions.115,116 Children who develop ocular toxocariasis are usually older and often do not have a history of prior systemic infestation. There is usually a history of pica and exposure to puppies.117,118 Vision loss occurs from damage to the vitreous and retina due to an inflammatory response to T. canis.119
Toxocara endophthalmitis may present in 3 classic forms: chronic endophthalmitis, posterior pole "granuloma," and peripheral inflammatory mass. There is no external inflammation in the chronic endophthalmitis form.120 An acute inflammation phase with associated anterior granulomatous response and yellowish-white infiltrates in the vitreous and retina may either subside or be followed by fibrocellular membrane development deep within the vitreous.121 Prognosis depends on the extent of intravitreous organization. The posterior pole granuloma form usually presents with strabismus. The vitreous is hazy with an ill-defined posterior pole mass that becomes well-defined as a gray granulomatous mass as the initial inflammation subsides (Figure 5). Visual prognosis is usually good with stable vision, although there is usually already some loss of central vision by the time of diagnosis.122 The peripheral inflammatory mass form may be preceded by acute diffuse endophthalmitis. As the inflammation subsides, a peripheral dense white mass becomes apparent, which is either diffuse or spherical.123 Prognosis is relatively good, although surgical treatment, such as scleral buckling and vitrectomy, may be required if there are associated intraretinal bands and resultant retinal detachment.124-126
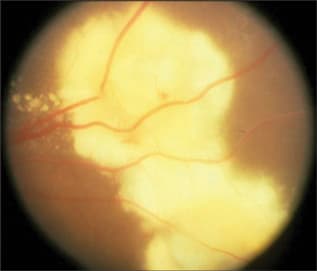
Figure 5. Toxocara canis retinitis.
The diagnosis of ocular toxocariasis is usually made by using serum and intraocular fluids for ELISA testing and cytology analysis.127-129 Patients frequently do not have serum eosinophilia, although the presence of eosinophils in aqueous humor or vitrectomy specimens suggests the infection.130 Treatment, depending on the stage and secondary effects of the disease, is controversial due to the theoretical risk of worsened inflammation when the intraocular organism is killed. For cases when the mobile larvae can be found, direct laser photocoagulation may be useful.131 Studies show the benefit of using albendazole or thiabendazole with topical or periocular injections of corticosteroids.132-134
OCULAR TUBERCULOSIS
Tuberculosis, an airborne infection caused by Mycobacterium tuberculosis, most commonly affects the lungs, although extrapulmonary manifestations are not uncommon. Histologically, tuberculous lesions are characterized by caseating granulomas.135 Among the extrapulmonary manifestations, intraocular tuberculosis is believed to result from hematogenous spread of the bacilli.136
The most common presentation is posterior uveitis followed by anterior uveitis and panuveitis (Figure 6).137 Tubercular retinal vasculitis is also common and is associated with vitreous infiltrates, retinal hemorrhage, neovascularization, and neuroretinitis.138-140 Posterior involvement can be divided into 4 forms: choroidal tubercles, choroidal tuberculoma, subretinal abscess, and serpiginous-like choroiditis. The most common is multiple choroidal tubercles, which appear as small grayish nodules in the posterior pole of one or both eyes (Figure 7). These usually respond well to treatment and take up to 4 months to heal.141-143 Choroidal tuberculoma, a less common presentation in which hemorrhages and retinal folds may be seen on the tuberculoma surface,144 may be misdiagnosed as an intraocular tumor.145-147 Subretinal abscesses are yellow necrotizing granulomas that usually heal with treatment and have a good prognosis.148,149 Serpiginous-like choroiditis is a recurrent inflammation that involves the choroid and progresses to the retina, despite systemic corticosteroids and immunosuppressive agents. Additionally, the fellow eye may be affected months or years later.150,151
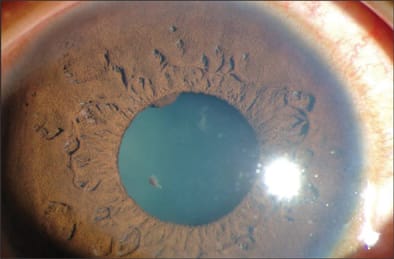
Figure 6. Granulomatous uveitis associated with intraocular tuberculosis. A Koeppe nodule is noted at the 11:00 position.
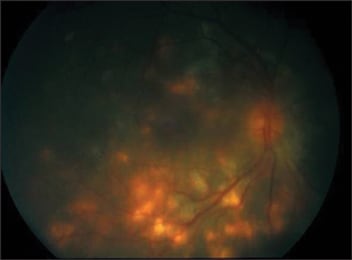
Figure 7. Tuberculous retinochoroiditis.
The diagnosis of intraocular tuberculosis should be suspected based on clinical grounds. These can be supported by a positive purified protein derivative skin testing and chest X-ray suggestive of pulmonary involvement.152 Newer diagnostic modalities include assessment of interferon-gamma release in assays such as QuantiFERON Gold TB test (Cellestis, Ltd., Carnegie, Australia).153 Direct isolation or demonstration of the acid-fast bacilli in the ocular fluid or tissue or the detection of the M. tuberculosis genome by PCR and other nucleic acid amplification techniques confirms the diagnosis of tuberculosis.154-158
The treatment of ocular tuberculosis is similar to that for pulmonary or extrapulmonary tuberculosis. This includes at least 3 drugs (isoniazid, rifampin, and pyrazinamide, with or without ethambutol) for 2 months, followed by isoniazid and rifampin for the next 7 months.159,160 Some studies have described treatment of ocular tuberculosis for 9 months with isoniazid and rifampin, although this is not ideal and currently not the standard of care.161-163 The final choice of antibiotic therapy should be guided by susceptibility testing. Second-line agents, such as streptomycin, capreomycin, and quinolones, are often reserved for cases due to multi–drug-resistant tuberculosis.164,165
OCULAR SYPHILIS
Ocular syphilis is caused either by the direct invasion of the spirochete Treponema pallidum or by an allergic reaction in tissues sensitized by the pathogen. Studies show that the incidence of ocular syphilis is on the rise over the past decade, possibly as the result of high-risk behavior associated with the spread of AIDS.166-168
Ocular syphilis has different manifestations depending on its time of onset. Congenital syphilis is usually associated with a pigmentary retinopathy that appears somewhat like retinitis pigmentosa. This retinopathy may be segmental or generalized, and it can present in either patients without any prior symptomatic inflammatory episodes or in those who have had an episode of syphilitic interstitial keratitis.169,170 In acquired syphilis, there is usually a patchy diffuse neuroretinitis that can have hemorrhagic areas. Flare and cells can be seen in the anterior and posterior segments. Clinically, there is reduced VA and contraction of the visual fields.171
Syphilis is diagnosed serologically with the rapid plasma reagin (RPR) test, followed by the more sensitive fluorescent treponemal antibody absorption test (FTA-ABS).172 Serum RPR can be negative in some cases of neuroretinitis despite a positive FTA-ABS test; thus, in such cases, a lumbar puncture can be useful to assess spinal fluid involvement. The primary treatment for syphilis is penicillin G. Ocular syphilis is often considered as a type of central nervous system disease and therefore, as with neurosyphilis, a high dose of 10 million units of penicillin given intravenously daily for 10 to 14 days is required.173 For penicillin-allergic patients, ceftriaxone and doxycycline are effective alternatives, although penicillin desensitization may be attempted, especially in pregnant women.174 Early treatment of syphilitic neuroretinitis can result in improvement of VA and expansion of the visual fields.175
CONCLUSIONS
Infectious retinitis represents a spectrum of ophthalmic diseases that are potentially preventable and treatable. The foregoing discussion of selected infectious retinitides illustrates the wide array of potential pathogens from viruses to fungi, bacteria, and parasites. It also highlights its occurrence in both immune-competent and immune-compromised hosts. While the pathogens and the hosts vary widely, prevention of the devastating outcome of vision loss is the uniform goal of management. In this regard, knowledge of the offending pathogen, its typical clinical manifestations, and its anti-infective susceptibility pattern are essential to successful treatment. Likewise, knowledge of the immune status of the host is essential, since immune-modifying strategies may be needed to complement the anti-infective treatment, because infectious retinitis is much more aggressive and has a poorer outcome in immune-compromised patients. Finally, recognizing that infectious retinitis is often a component of a more systemic illness is important in the successful management of the disease. RP
REFERENCES
- Stagno S, Reynolds DW, Amos CS, et al. Auditory and visual defects resulting from symptomatic and subclinical congenital cytomegaloviral and toxoplasma infections. Pediatrics. 1977;59:669-678.
- Conboy TJ, Pass RF, Stagno S, et al. Early clinical manifestations and intellectual outcome in children with symptomatic congenital cytomegalovirus infection. J Pediatr. 1987;111:343-348.
- Murray HW, Knox DL, Green WR, et al. Cytomegalovirus retinitis in adults. A manifestation of disseminated viral infection. Am J Med. 1977;63:574-584.
- Oka S, Nagata Y, Fujino Y, et al. CD8+ T lymphocyte counts as an adjunctive predictor of cytomegalovirus retinitis in patients with acquired immunodeficiency syndrome. Intern Med. 1997;36:461-465.
- Shimakawa M, Kono C, Nagai T, et al. CMV retinitis after renal transplantation. Transplant Proc. 2002;34:1790-1792.
- Kuo IC, O'Brien TP, Broman AT, Ghajarnia M, Jabbur NS. Clinical characteristics and outcomes of cytomegalovirus retinitis in persons without human-immunodeficiency virus infection. Am J Ophthalmol. 2004;138:338-346.
- Pepose JS, Holland GN, Nestor MS et al. Acquired immune deficiency syndrome. Pathogenic mechanisms of ocular disease. Ophthalmology. 1985;92:472-484.
- Studies of Ocular Complications of AIDS Research Group in collaboration with the AIDS Clinical Trial Group. Foscarnet-Ganciclovir Cytomegalovirus Retinitis Trial: 5. Clinical features of cytomegalovirus retinitis at diagnosis. Am J Ophthalmol. 1997;124:141-157.
- Patel SS, Rutzen AR, Marx JL, et al. Cytomegalovirus papillitis in patients with acquired immune deficiency syndrome. Visual prognosis of patients treated with ganciclovir and/or foscarnet. Ophthalmology. 1996;103:1476-1482.
- Holland GN, Vaudaux JD, Jeng SM, et al. Characteristics of untreated AIDS-related cytomegalovirus retinitis. I. Findings before the era of highly active antiretroviral therapy (1988 to 1994). Am J Ophthalmol. 2008;145:5-11.
- Holland GN, Buhles WC Jr, Mastre B, et al. A controlled retrospective study of ganciclovir treatment for cytomegalovirus retinopathy. Use of a standardized system for the assessment of disease outcome. UCLA CMV Retinopathy. Study Group. Arch Ophthalmol. 1989;107:1759-1766.
- Jabs DA, Enger C, Haller J, et al. Retinal detachments in patients with cytomegalovirus retinitis. Arch Ophthalmol. 1991;109:794-799.
- Holland GN, Tufail A, Jordan MC. Cytomegalovirus diseases. In: Pepose JS, Holland GN, Wilhelmus KR, eds. Ocular Infection & Immunity. St. Louis: Mosby, 1996;1088-1129.
- Henderly DE, Freeman WR, Causey DM, et al. Cytomegalovirus retinitis and response to therapy with ganciclovir. Ophthalmology. 1987;94:425-434.
- Palestine AG, Rodrigues MM, Macher AM, et al. Ophthalmic involvement in acquired immunodeficiency syndrome. Ophthalmology. 1984;91:1092-1099.
- Rothova A, de Boer JH, Ten Dam-van Loon NH, et al. Usefulness of aqueous humor analysis for the diagnosis of posterior uveitis. Ophthalmology. 2008;115:306-311.
- McCann JD, Margolis TP, Wong MG, et al. A sensitive and specific polymerase chain reaction-based assay for the diagnosis of cytomegalovirus retinitis. Am J Ophthalmol. 1995;120:219-226.
- Perry CM, Balfour JA. Fomivirsen. Drugs. 1999;57:375-380; discussion 381.
- Schwetz BA: From the Food and Drug Administration. JAMA. 2001;285:2705.
- Martin DF, Parks DJ, Mellow SD, et al. Treatment of cytomegalovirus retinitis with an intraocular sustained-release ganciclovir implant. A randomized controlled clinical trial. Arch Ophthalmol. 1994;112:1531-1539.
- Musch DC, Martin DF, Gordon JF, et al. Treatment of cytomegalovirus retinitis with a sustained-release ganciclovir implant. The Ganciclovir Implant Study Group. N Engl J Med. 1997;337:83-90.
- Studies of Ocular Compliations of AIDS Research Group in collaboration with the AIDS Clinical Trials Group. Mortality in patients with the acquired immunodeficiency syndrome treated with either foscarnet or ganciclovir for cytomegalovirus retinitis. N Engl J Med. 1992;326:213-220.
- Lalezari JP, Stagg RJ, Kuppermann BD, et al. Intravenous cidofovir for peripheral cytomegalovirus retinitis in patients with AIDS. A randomized, controlled trial. Ann Intern Med. 1997;126:257-263.
- Vitravene Study Group. Randomized dose-comparison studies of intravitreous fomivirsen for treatment of cytomegalovirus retinitis that has reactivated or is persistently active despite other therapies in patients with AIDS. Am J Ophthalmol. 2002;133:475-483.
- Vitravene Study Group. A randomized controlled clinical trial of intravitreous fomivirsen for treatment of newly diagnosed peripheral cytomegalovirus retinitis in patients with AIDS. Am J Ophthalmol. 2002;133:467-474.
- Drew WL, Miner RC, Busch DF, et al. Prevalence of resistance in patients receiving ganciclovir for serious cytomegalovirus infection. J Infect Dis. 1991;163:716-719.
- Jabs DA, Enger C, Forman M, et al. Incidence of foscarnet resistance and cidofovir resistance in patients treated for cytomegalovirus retinitis. The Cytomegalovirus Retinitis and Viral Resistance Study Group. Antimicrob Agents Chemother. 1998;42:2240-2244.
- Karavellas MP, Lowder CY, Macdonald C, et al. Immune recovery vitritis associated with inactive cytomegalovirus retinitis: a new syndrome. Arch Ophthalmol. 1998;116:169-175.
- Zegans ME, Walton RC, Holland GN, et al. Transient vitreous inflammatory reactions associated with combination antiretroviral therapy in patients with AIDS and cytomegalovirus retinitis. Am J Ophthalmol. 1998;125:292-300.
- Song MK, Azen SP, Buley A, et al. Effect of anti-cytomegalovirus therapy on the incidence of immune recovery uveitis in AIDS patients with healed cytomegalovirus retinitis. Am J Ophthalmol. 2003;136:696-702.
- Culbertson WW, Blumenkranz MS, Pepose JS, et al. Varicella zoster virus is a cause of the acute retinal necrosis syndrome. Ophthalmology. 1986;93:559-569.
- Ganatra JB, Chandler D, Santos C, et al. Viral causes of the acute retinal necrosis syndrome. Am J Ophthalmol. 2000;129:166-172.
- Itoh N, Matsumura N, Ogi A, et al. High prevalence of herpes simplex virus type 2 in acute retinal necrosis syndrome associated with herpes simplex virus in Japan. Am J Ophthalmol. 2000;129:404-405.
- Urayama A, Yamada N, Sasaki T, et al. Unilateral acute uveitis with retinal periarteritis and detachment. Rinsho Ganka. 1971;25:607-619.
- Young NJ, Bird AC. Bilateral acute retinal necrosis. Br J Ophthalmol. 1978;62:581-590.
- Fisher JP, Lewis ML, Blumenkranz M, et al. The acute retinal necrosis syndrome. Part 1: Clinical manifestations. Ophthalmology. 1982;89:1309-1316.
- Margolis R, Brasil OF, Lowder CY, et al. Multifocal posterior necrotizing retinitis. Am J Ophthalmol. 2007;143:1003-1008.
- Usui Y, Goto H. Overview and diagnosis of acute retinal necrosis syndrome. Semin Ophthalmol. 2008;23:275-283.
- Knox CM, Chandler D, Short GA, et al. Polymerase chain reaction-based assays of vitreous samples for the diagnosis of viral retinitis. Use in diagnostic dilemmas. Ophthalmology. 1998;105:37-44 (discussion 44-5).
- de Boer JH, Verhagen C, Bruinenberg M, et al. Serologic and polymerase chain reaction analysis of intraocular fluids in the diagnosis of infectious uveitis. Am J Ophthalmol. 1996;121:650-658.
- Holland GN. The progressive outer retinal necrosis syndrome. Int Ophthalmol. 1994;18:163-165.
- Roig-Melo EA, Macky TA, Heredia-Elizondo ML, et al. Progressive outer retinal necrosis syndrome: successful treatment with a new combination of antiviral drugs. Eur J Ophthalmol. 2001;11:200-202.
- Kim SJ, Equi R, Belair ML, Fine HF, et al. Long-term preservation of vision in progressive outer retinal necrosis treated with combination antiviral drugs and highly active antiretroviral therapy. Ocul Immunol Inflamm. 2007;15:425-427.
- Muthiah MN, Michaelides M, Child CS. Acute retinal necrosis: a national population-based study to assess the incidence, methods of diagnosis, treatment strategies and outcomes in the UK. Br J Ophthalmol. 2007;91:1452-1455.
- Blumenkranz MS, Culbertson WW, Clarkson JG, et al. Treatment of the acute retinal necrosis syndrome with intravenous acyclovir. Ophthalmology. 1986;93:296-300.
- Figueroa MS, Garabito I, Gutierrez C, et al. Famciclovir for the treatment of acute retinal necrosis (ARN) syndrome. Am J Ophthalmol. 1997;123:255-257.
- Aslanides IM, De Souza S, Wong DT, et al. Oral valaciclovir in the treatment of acute retinal necrosis syndrome. Retina. 2002;22:352-354.
- Blumenkranz MS, Duker JS, D'Amico DJ. Acute retinal necrosis. In: Albert DM, Jackobiec FA (Eds.). Principles and practice of ophthalmology: Clinical Practice. Vol 2. Philadelphia, PA: WB Saunders, 1994;Chapter 78.
- Ando F, Kato M, Goto S, et al. Platelet function in bilateral acute retinal necrosis. Am J Ophthalmol. 1983;96:27-32.
- Culbertson WW, Atherton SS. Acute retinal necrosis and similar retinitis syndrome. Int Ophthalmol Clin. 1993;33:129-143.
- Lau CH, Missotten T, Salzmann J, et al. Acute retinal necrosis features, management, and outcomes. Ophthalmology. 2007;114:756-762.
- Kawaguchi T, Spencer DB, Mochizuki M. Therapy for acute retinal necrosis. Semin Ophthalmol. 2008;23:285-290.
- McDonald HR, Lewis H, Kreiger AE, et al. Surgical management of retinal detachment associated with the acute retinal necrosis syndrome. Br J Ophthalmol. 1991;75:455-458.
- Chen HP, Kuo HK, Tsai SH, et al. Acute retinal necrosis syndrome: clinical manifestations and visual outcomes. Chang Gung Med J. 2004;27:193-200.
- Pettit TH, Edwards JE, Purdy EP, et al. Endogenous fungal endophthalmitis. In: Pepose JS, Holland GN, Wilhelmus KR, eds. Ocular Infection and Immunity. St Louis, MO: Mosby, 1996;1262-1285.
- Joshi N, Hamory BH. Endophthalmitis caused by non-albicans species of Candida. Rev Infect Dis. 1991;13:281-287.
- Griffin JR, Pettit TH, Fishman LS, et al. Blood-borne Candida endophthalmitis. A clinical and pathologic study of 21 cases. Arch Ophthalmol. 1973;89:450-456.
- Edwards JE Jr, Foos RY, Montgomerie JZ, et al. Ocular manifestations of Candida septicemia: a review of seventy-six cases of hematogenous Candida endophthalmitis. Medicine (Baltimore) 1974;53:47-75.
- Graham E, Chignell AH, Eykyn S. Candida endophthalmitis: a complication of prolonged intravenous therapy and antibiotic treatment. J Infect. 1986;13:167-173.
- Michelson PE, Stark W, Reeser F, et al. Endogenous Candida endophthalmitis. Report of 13 cases and 16 from the literature. Int Ophthalmol Clin. 1971;11:125-147.
- Dupont B, Drouhet E. Cutaneous, ocular, and osteoarticular candidiasis in heroin addicts: new clinical and therapeutic aspects in 38 patients. J Infect Dis. 1985;152:577-591.
- Servant JB, Dutton GN, Ong-Tone L, et al. Candidal endophthalmitis in Glaswegian heroin addicts: report of an epidemic. Trans Ophthalmol Soc U K. 1985;104:297-308.
- Palmer EA. Endogenous Candida endophthalmitis in infants. Am J Ophthalmol. 1980;89:388-395.
- Baley JE, Annable WL, Kliegman RM. Candida endophthalmitis in the premature infant. J Pediatr. 1981;98:458-461.
- Aguilar GL, Blumenkrantz MS, Egbert PR, et al. Candida endophthalmitis after intravenous drug abuse. Arch Ophthalmol. 1979;97:96-100.
- Doft BH, Clarkson JG, Rebell G, et al. Endogenous Aspergillus endophthalmitis in drug abusers. Arch Opthalmol. 1980;98:859-862.
- Demicco DD, Reichman RC, Violette EJ, et al. Disseminated aspergillosis presenting with endophthalmitis. A case report and review of the literature. Cancer. 1984;53:1995-2001.
- Naidoff MA, Green WR. Endogenous aspergillus endophthalmitis occurring after kidney transplant. Am J Ophthalmol. 1975;79:502-509.
- Riddell IJ, McNeil SA, Johnson TM, et al. Endogenous Aspergillus endophthalmitis: a report of 3 cases and review of the literature. Medicine (Baltimore) 2002;81:311-320.
- Essman TF, Flynn HW Jr, Smiddy WE, et al. Treatment outcomes in a 10-year study of endogenous fungal endophthalmitis. Ophthalm Surg Lasers. 1997;28:185-194.
- Jampol LM, Dyckman S, Maniates V, et al. Retinal and choroidal infarction from Aspergillus: clinical diagnosis and clinicopathologic correlations. Trans Am Ophthalmol Soc. 1998;86:422-440.
- Weishaar PD, Flynn HW Jr, Murray TG, et al. Endogenous Aspergillus endophthalmitis. Clinical features and treatment outcomes. Opthalmolgy. 1998;105:57-65.
- Schuman JS, Friedman AH. Retinal manifestations of the acquired immunodeficiency syndrome (AIDS): cytomegalovirus, Candida albicans, Cryptococcus, toxoplasmosis and Pneumocystis carinii. Trans Ophthalmol Soc U K. 1983;103:177-190.
- Carney MD, Combs JL, Waschler W. Cryptococcal choroiditis. Retina. 1990;10:27-32.
- Winward KE, Hamed LM, Glaser JS. The spectrum of optic nerve disease in human immunodeficiency virus infection. Am J Ophthalmol. 1989;107:373-380.
- Crump JR, Elner SG, Elner VM, et al. Cryptococcal endophthalmitis: case report and review. Clin Infect Dis. 1992;14:1069-1073.
- Hiss PW, Shields JA, Augsburger JJ. Solitary retinovitreal abscess as the intial manifestation of cryptococcosis. Ophthalmology. 1988;95:162-165.
- Sheu SJ, Chen YC, Kuo NW, et al. Endogenous cryptococcal endophthalmitis. Ophthalmology. 1998;105:377-381.
- Morinelli EN, Dugel PU, Riffenburgh R, et al. Infectious multifocal choroiditis in patients with acquired immune deficiency syndrome. Ophthalmology. 1993;100:1014-1021.
- Henderly DE, Liggitt PE, Rao NA. Cryptococcal chorioretinitis and endophthalmitis. Retina. 1987;7:75-79.
- Shields JA, Wright DM, Augsurger JJ, et al. Cryptococcal chorioretinitis. Am J Ophthalmol. 1980;89:210-217.
- Donahue SP, Hein E, Sinatra RB. Ocular involvement in children with candidemia. Am J Ophthalmol. 2003;135:886-887.
- Scherer WJ, Lee K. Implications of early systemic therapy on the incidence of endogenous fungal endophthalmitis. Ophthalmology. 1997;104:1593-1598.
- Brod RD, Flynn HW Jr, Clarkson JG, et al. Endogenous Candida endophthalmitis. Management without intravenous amphotericin B. Ophthalmology. 1990;96:666-672.
- Medoff G, Kobayashi GS. Strategies in the treatment of systemic fungal infections. N Engl J Med. 1980;302:145-155.
- Edwards JE, Jr., Lehrer RI, Stiehm ER, et al. Severe candidal infections: clinical perspective, immune defense mechanisms, and current concepts of therapy. Ann Intern Med. 1978;89:91-106.
- Shah CP, McKey J, Spirn MJ, et al. Ocular candidiasis: a review. Br J Ophthalmol. 2008;92:466-468.
- Ackler ME, Vellend H, McNeely DM, et al. Use of fluconazole in the treatment of candidal endophthalmitis. Clin Infect Dis. 1995;20:657-664.
- Nomura J, Ruskin J. Failure of therapy with fluconazole for candidal endophthalmitis. Clin Infect Dis. 1993;17:888-889.
- Ohnishi Y, Tawara A, Murata T, et al. Postmortem findings two weeks after oral treatment for metastatic Candida endophthalmitis with fluconazole. Ophthalmologica. 1999;213:341-344.
- Gao H, Pennesi ME, Shah K, et al. Intravitreal voriconazole: an electroretinographic and histopathological study. Arch Ophthalmol 2004;122:1687-1692.
- Hariprasad SM, Mieler WF, Lin TK, et al. Voriconazole in the treatment of fungal eye infections: a review of current literature. Br J Ophthalmol. 2008;92:871-878.
- Narendran N, Balasubramaniam B, Johnson E, et al. Five-year retrospective review of guideline-based management of fungal endophthalmitis. Acta Ophthalmol. 2008;86:525-532.
- Breit SM, Hariprasad SM, Mieler WF, et al. Management of endogenous fungal endophthalmitis with voriconazole and caspofungin. Am J Ophthalmol. 2005;139:135-140.
- Martinez-Vazquez C, Fernandez-Ulloa J, Bordon J, et al. Candida albicans endophthalmitis in brown heroin addicts: response to early vitrectomy preceded and followed by antifungal therapy. Clin Infec Dis. 1998;27:1130-1133.
- Snip RC, Michels RG. Pars plana vitrectomy in the management of endogenous Candida endophthalmitis. Am J Ophthalmol. 1976;82:699-704.
- Teutsch SM, Juranek DD, Sulzer A, et al. Epidemic toxoplasmosis associated with infected cats. N Engl J Med. 1979;300:695-699.
- Miller NL, Frenkel JK, Dubey JP. Oral infections with Toxoplasma cysts and oocytes in felines, other mammals, and in birds. J Parasitol. 1972;58:928-937.
- Fenkel JK. Pathogenesis of toxoplasmosis with a consideration of cyst rupture in Besnoitia infection. Surv Ophthalmol. 1961;6:799-832.
- Frenkel JK, Jacobs L. Ocular toxoplasmosis: pathogenesis, diagnosis, and treatment. Arch Ophthalmol. 1958;59:260-279.
- Abrahams IW, Gregerson DS. Longitudinal study of serum antibody responses to retinal antigens in acute ocular toxoplasmosis. Am J Ophthalmol. 1982;93:224-231.
- Hausmann N, Richard G. Acquired ocular toxoplasmosis: a fluroscein angiography study. Ophthalmology. 1991;98:1647-1651.
- Folk JC, Lobes LA. Presumed toxoplasmic papillitis. Ophthalmology. 1984;91:64-67.
- Nussenblatt RB, Belfort R Jr. Ocular toxoplasmosis. JAMA. 1994;271:304-309.
- Shepp DH, Hackman RC, Conley FK, et al. Toxoplasma gondii reactivation identified by detection of parasitemia in tissue culture. Ann Intern Med. 1985;103:218-221.
- Rothova A, Meenken C, Buitenhuis HJ, et al. Therapy for ocular toxoplasmosis. Am J Ophthalmol. 1993;115:517-523.
- Soheilian M, Sadoughi MM, Ghajarnia M, et al. Prospective randomized trial of trimethoprim/sulfamethoxazole versus pyrimethamine and sulfadiazine in the treatment of ocular toxoplasmosis. Ophthalmology. 2005;112:1876-1882.
- Bosch-Driessen LH, Verbraak FD, Suttorp-Schulten MS, et al. A prospective, randomized trial of pyrimethamine and azithromycin vs pyrimethamine and sulfadiazine for the treatment of ocular toxoplasmosis. Am J Ophthalmol. 2002;134:34-40.
- Silveira C, Belfort R Jr, Muccioli C, et al. The effect of long-term intermittent trimethoprin-sulfamethoxazole treatment on recurrences of toxoplasmic retinochoroiditis. Am J Ophthalmol. 2002;134:41-46.
- Ongkosuwito JV, Bosch-Driessen EH, Kijlstra A, et al. Serologic evaluation of patients with primary and recurrent ocular toxoplasmosis for evidence of recent infection. Am J Ophthalmol. 1999;128:407-412.
- Bonfioli AA, Orefice F. Toxoplasmosis. Semin Ophthalmol. 2005;20:129-141.
- Altcheh J, Nallar M, Conca M, et al. Toxocariasis: clinical and laboratory features in 54 patients. Ann Pediatr (Barcelona). 2003;58:425-431.
- Ellis GS Jr, Pakalnis VA, Worley G, et al. Toxocara canis infestation. Clinical and epidemiological associations with seropositivity in kindergarten children. Ophthalmology. 1986;93:1032-1037.
- Espinoza YA, Huapaya PH, Roldán WH, et al. Clinical and serological evidence of Toxocara infection in school children from Morrope district, Lambayeque, Peru. Rev Inst Med Trop Sao Paulo. 2008;50:101-105.
- Molk R. Ocular toxocariasis: a review of the literature. Ann Ophthalmol. 1983;15:216-231.
- Glickman LT, Magnaval J. Zoonotic roundworm infections. Infect Dis Clin North Am. 1993;7:717-732.
- Marmor M, Glickman L, Shofer F, et al. Toxocara canis infection of children: epidemiologic and neuropsychologic findings. Am J Public Health. 1987;77:554-559.
- Schantz PM, Meyer D, Glickman LT. Clinical, serologic, and epidemiologic characteristics of ocular toxocariasis. Am J Trop Med Hyg. 1979;28:24-28.
- Shields JA. Ocular toxocariasis: a review. Surv Ophthalmol. 1984;28:361-381.
- Wilkinson CP, Welch RB. Intraocular toxocara. Am J Ophthalmol. 1971;71:921-930.
- Wan WL, Cano MR, Pince KJ, et al. Echographic characteristics of ocular toxocariasis. Ophthalmology. 1991;98:28-32.
- Monshizadeh R, Ashrafzadeh MT, Rumelt S. Choroidal neovascular membrane: a late complication of inactive Toxocara chorioretinitis. Retina. 2000;20:219-220.
- Hogan MJ, Kimura SJ, Spencer WH. Visceral larva migrans and peripheral retinitis. JAMA. 1965;194:1345-1347.
- Hagler WS, Pollard ZF, Jarrett WH, et al. Results of surgery for ocular Toxocara canis. Ophthalmology. 1981;88:1081-1086.
- Amin HI, McDonald HR, Han DP, et al. Vitrectomy update for macular traction in ocular toxocariasis. Retina. 2000;20:80-85.
- Small KW, McCuen BW 2nd, de Juan E Jr, et al. Surgical management of retinal traction caused by toxocariasis. Am J Ophthalmol. 1989;108:10-14.
- Biglan AW, Glickman LT, Lobes LA Jr. Serum and vitreous Toxocara antibody in nematode endophthalmitis. Am J Ophthalmol. 1979;88:898-901.
- Saporito L, Scarlata F, Colomba C, et al. Human toxocariasis: a report of nine cases. Acta Paediatr. 2008;97:1301-1302.
- de Visser L, Rothova A, de Boer JH, et al. Diagnosis of ocular toxocariasis by establishing intraocular antibody production. Am J Ophthalmol. 2008;145:369-374.
- Sharkey JA, McKay PS. Ocular toxocariasis in a patient with repeatedly negative ELISA titre to Toxocara canis. Br J Ophthalmol. 1993;77:253-254.
- Sorr EM: Meandering ocular toxocariasis. Retina. 1984;4:90-96.
- O'Connor GR. Chemotherapy of toxoplasmosis and toxocariasis. In: Srinivasan BD, ed. Ocular Therapeutics. New York, NY: Masson;1980.
- Barisani-Asenbauer T, Maca SM, Hauff W, et al. Treatment of ocular toxocariasis with albendazole. J Ocul Pharmacol Ther. 2001;17:287-294.
- Stürchler D, Schubarth P, Gualzata M, et al. Thiabendazole vs. albendazole in treatment of toxocariasis: a clinical trial. Ann Trop Med Parasitol. 1989;83:473-478.
- Centers for Disease Control and Prevention. Case definitions for infectious conditions under public health surveillance. MMWR Morb Mortal Wkly Rep. 1997;46:1-55.
- Golden MP, Vikram HR. Extrapulmonary tuberculosis: an overview. Am Fam Physician. 2005;72:1761-1768.
- Gupta V, Gupta A, Rao NA. Intraocular tuberculosis — an update. Surv Ophthalmol. 2007;52:561-587.
- Gupta A, Gupta V, Arora S, et al. PCR-positive tubercular retinal vasculitis: clinical characteristics and management. Retina. 2001;21:435-444.
- Hoh HB, Kong VY, Jaais F. Tuberculous retinal vasculitis. Med J Malaysia. 1998;53:288-289.
- Rosen PH, Spalton DJ, Graham EM. Intraocular tuberculosis. Eye. 1990;4:486-492.
- Massaro D, Katz S, Sachs M. Choroidal tubercles. A clue to hematogenous tuberculosis. Ann Inter Med. 1964;60:231-241.
- Olazabal F. Choroidal tubercles. a neglected sign. JAMA. 1967;200:74-77.
- Tejada P, Mendez MJ, Negreira S. Choroidal tubercles with tuberculous meningitis. Int Ophthalmol. 1994;18:115-118.
- Cangemi FE, Friedman AH, Josephberg R. Tuberculoma of the choroid. Ophthalmology. 1980;87:252-258.
- Demirci H, Shields CL, Shields JA, et al. Ocular tuberculosis masquerading as ocular tumors. Surv Ophthalmol. 2004;49:78-89.
- Sant MS. Ocular tuberculosis masquerading as retinoblastoma. Indian J Pathol Microbiol. 1994;37:343-347.
- Sharma PM, Singh RP, Kumar A, et al. Choroidal tuberculoma in miliary tuberculosis. Retina. 2003;23:101-104.
- Mason JO. Treatment of large macular choroidal tubercle improves vision. Arch Ophthalmol. 2000;118:1136-1137.
- Wang JC, Chuah GC, Yap EY. Tuberculous choroidal granulomas in a patient with systemic lupus erythematosus. A case report. Int Ophthalmol. 2001;24:107-109.
- Laatikainen L, Erkkilä H. Serpiginous choroiditis. Br J Ophthalmol. 1974;58:777-783.
- Gupta V, Gupta A, Arora, S et al. Presumed tubercular serpiginouslike choroiditis: clinical presentations and management. Ophthalmology. 2003;110:1744-1749.
- Rossman MD, Maylock RL. Pulmonary tuberculosis. In: Schlossberg D, ed. Tuberculous and Nontuberculous Mycobacterial Infections. Philadelphia, PA: W.B. Saunders Co, 1999;143-153.
- Pai M, Kalantri S, Dheda K. New tools and emerging technologies for the diagnosis of tuberculosis: part I. Latent tuberculosis. Expert Rev Mol Diagn. 2006;6:413-422.
- Biswas J, Madhavan HN, Gopal L, et al. Intraocular tuberculosis. Clinicopathologic study of five cases. Retina. 1995;15:461-468.
- Arora SK, Gupta V, Gupta A, et al. Diagnostic efficacy of polymerase chain reaction in granulomatous uveitis. Tuber Lung Dis. 1999;79:229-233.
- Barondes MJ, Sponsel WE, Stevens TS, et al. Tuberculous choroiditis diagnosed by chorioretinal endobiopsy. Am J Ophthalmol. 1991;112:460-461.
- Johnston RL, Tufail A, Lightman S, et al. Retinal and choroidal biopsies are helpful in unclear uveitis of suspected infectious or malignant origin. Ophthalmology. 2004;111:522-528.
- Salman A, Parmar P, Rajamohan M, et al. Subretinal fluid analysis in the diagnosis of choroidal tuberculosis. Retina. 2003;23:796-799.
- Centers for Disease Control. Treatment of Tuberculosis. American Thoracic Society, CDC, and Infectious Diseases Society of America, MMWR Morb Mortal Wkly Rep. 2003;52:RR1.
- Kuruvilla A. Ocular tuberculosis. Lancet. 2003;361:260-261.
- Kratka WH. Isoniazid and ocular tuberculosis: an evaluation of experimental and clinical studies. AMA Arch Ophthalmol. 1995;54:330-344.
- Morimura Y, Okada AA, Kawahara S, et al. Tuberculin skin testing in uveitis patients and treatment of presumed intraocular tuberculosis in Japan. Ophthalmology. 2002;109:851-857.
- Schlaegel TF, Weber JC. Double-blind therapeutic trial of isoniazid in 344 patients with uveitis. Br J Ophthalmol. 1969;53:425-427.
- Vrioni G, Levidiotou S, Matsiota-Bernard P. Molecular characterization of Mycobacterium tuberculosis isolates presenting various drug susceptibility from Greece using three DNA typing methods. J Infect. 2004;48:253-262.
- Patterson PE, Kimerling ME, Bailey WC, et al. Chemotherapy of tuberculosis, Schlossberg D, ed. Tuberculous and Nontuberculous Mycobacterial Infections. 4th ed. Philadelphia, PA: W.B. Saunders Company, 1999;71-82.
- Doris JP, Saha K, Jones NP, et al. Ocular syphilis: the new epidemic. Eye. 2006;20:703-705.
- Chao JR, Khurana RN, Fawzi AA, et al. Syphilis: reemergence of an old adversary. Ophthalmology. 2006;113:2074-2079.
- Parc CE, Chahed S, Patel SV, et al. Manifestations and treatment of ocular syphilis during an epidemic in France. Sex Transm Dis. 2007;34:553-556.
- Boot JM, Oranje AP, de Groot R, et al. Congenital syphilis. Int J STD AIDS 1992;3:161-167.
- Probst LE, Wilkinson J, Nichols BD. Diagnosis of congenital syphilis in adults presenting with interstitial keratitis. Can J Ophthalmol. 1994;29:77-80.
- Margo CE, Hamed LM. Ocular syphilis. Surv Ophthalmol. 1992;37:203-220.
- Kent ME, Romanelli F. Reexamining syphilis: an update on epidemiology, clinical manifestations, and management. Ann Pharmacother. 2008;42:226-236.
- Browning DJ. Posterior segment manifestations of active ocular syphilis, their response to a neurosyphilis regimen of penicillin therapy, and the influence of human immunodeficiency virus status on response. Ophthalmology. 2000;107:2015-2023.
- Goldmeier D, Hay P. A review and update on adult syphilis, with particular reference to its treatment. Int J STD AIDS. 1993;4:70-82.
- Tamesis RR, Foster CS. Ocular syphilis. Ophthalmology. 1990;97:1281-1287.