







Combination Therapy for Choroidal Neovascularization
ALBERT J. AUGUSTIN, MD
Parallel with the introduction of new, potent monotherapies for choroidal neovascularization (CNV), we are facing a clear trend toward individualized medicine. With CNV, this may mean combination therapy. Various US populations confirm that the prevalence of age-related macular degeneration (AMD) increases with age.1-4 The prevalence of AMD in the US population ≥40 years old is estimated at 1.47% (1.75 million cases), and the number of cases is expected to increase by 50% to 2.95 million by 2020.1 Western Europe is estimated to have 3.35 million cases of AMD, and Australia has 130,000 cases.1
DRAWBACKS OF COMBINATION THERAPY
All relevant available treatments for CNV have drawbacks as monotherapies. These therapies include photodynamic therapy (PDT) with verteporfin (Visudyne, QLT/Novartis) and anti-vascular endothelial growth factor (VEGF) therapies (ranibizumab [Lucentis, Genentech], bevacizumab [Avastin, Genentech], and pegaptanib sodium [Macugen, OSI/Pfizer]), which have been evaluated primarily in patients with CNV due to AMD (ie, patients age 50 years or older).
Thus, several monotherapies are available for CNV, but none is perfect. PDT, pegaptanib, and anecortave acetate (Retaane, Alcon) do not improve vision in most patients. Ranibizumab improves vision, but continuous monthly intravitreal injections are required to maintain improved vision. Bevacizumab is believed to improve vision based on its similarity to ranibizumab, but it also appears to require monthly or 6-week injections. A need for practical combination therapy exists to address these shortcomings of monotherapy.
Combination therapy for CNV is derived from the combination therapy concept in oncology. In both therapeutic areas (oncology and ophthalmology), the goal of combination therapy is to disrupt the multiple stimuli that lead to pathologic cellular proliferation. In cancer, tumors and the neovasculature that feeds the tumors are targets, while in CNV, the neovasculature itself is the target.
Numerous factors have been identified as being important in the pathogenesis of CNV due to AMD. Most notably, the role of inflammation and genetic predisposition to inflammation is being elucidated. Complement factor H polymorphism also appears to be associated with AMD pathogenesis.5-8
The 3 main therapeutic targets of CNV development and proliferation are therefore the established neovascularization, angiogenesis, and inflammation. A current therapy that addresses these targets is the combination of verteporfin plus PDT to eradicate established CNV, an anti-VEGF therapy to block angiogenesis, and an anti-inflammatory approach to stop inflammation. The rationale for combination therapy with 2 or all 3 of these agents has been described in detail.9-12
Several trials provide evidence for the efficacy of combination therapies. First, verteporfin plus PDT was combined with intravitreal triamcinolone acetonide (TA). Available data for this combination were reviewed in 200513 and 2006.14 The major drawback of this approach was the relatively high risk of increased intraocular pressure, which may occur as late as 9 months after therapy. With the introduction of intravitreal anti-VEGF therapies for CNV, the opportunity arose for combination therapy that would provide better vision outcomes and safety profile than the PDT plus TA combination.
PATIENTS AND METHODS IN OUR CASE SERIES
In a prospective case series, researchers evaluated 104 patients with CNV due to AMD who were treated with a combination of PDT plus intravitreal bevacizumab (1.5 mg) and dexamethasone (0.8 mg).11 Reduced-fluence PDT (42 J/cm2 given at the standard fluence rate of 600 mW/cm2 for a reduced time of 70 seconds) was administered 16 hours before bevacizumab and dexamethasone injections.
RESULTS
Patients attended follow-up visits every 6 weeks. After an average follow-up of 62 weeks, the mean increase in visual acuity (VA) was 1.78 lines (8.9 letters; P<.01). Thirty-nine percent of patients had VA improved by at least 3 lines. Mean decrease in central retinal thickness was 171 μm (P<.01). No serious adverse events were observed. The Figure shows a clinical example from this series.
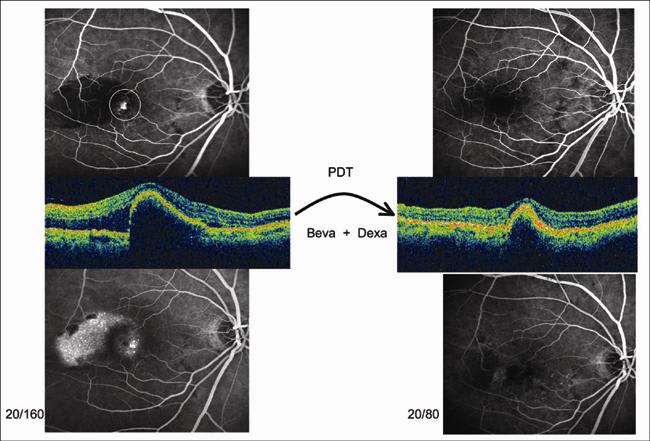
IMAGE APPEARS COURTESY OF THE AUTHOR.
Figure 1. Small classic lesion with a large RPE detachment Left: early and late phase angiography and OCT before therapy; right: early- and late-phase angiography and OCT >12 months after therapy. Circle indicates the PDT-treated area. VA increased from 20/160 to 20/80. Follow-up is more than 12 months in this case. Only 1 treatment was necessary to achieve a complete regression.
In addition to these published studies, results from several other studies have been presented at scientific meetings. These preliminary results have revealed good vision outcomes and/or lower retreatment rates, good safety profiles, and/or favorable morphological effects for double therapies15-17 and triple therapies18,19 with anti-VEGF, PDT, and (for triple therapy) steroid combinations. The ideal AMD therapy would improve vision safely and conveniently (ideally 1 treatment). Based on current data, combination therapy, and triple therapy in particular, as described above comes the closest to meeting this goal.
With different therapies, doses, timing, and treatment sequences possible for treating CNV, conducting definitive large randomized trials to determine the best therapy or combination therapy becomes cumbersome if not impossible. The multiplicity of therapies for CNV is a blessing and a challenge: we have many options to offer patients, but we do not know which option offers the greatest risk/benefit/feasibility profile.
Variability of patients and disease manifestation further complicate treatment choices. Disease characteristics, such as CNV predominance and morphology, highly variable VEGF values, and varied inflammatory drivers, may ultimately have important implications for choosing a treatment.
No therapy can claim a cure for CNV. Ultimately, the underlying cause of the disease remains unknown. Nevertheless, combination therapy with PDT and ranibizumab or bevacizumab anti-VEGF therapy appears be effective in eradicating CNV, such that vision improvement is comparable to that with ranibizumab monotherapy with fewer retreatments. The addition of a steroid component to target inflammation may provide better longevity of vision improvement so that even fewer retreatments are needed. This is our experience with triple therapy using PDT, bevacizumab, and dexamethasone; in most cases, only 1 treatment was required to maintain vision improvement of nearly 2 lines over a 10-month period.11
CONCLUSION
Definitive studies are still necessary, but multiple options for therapy remain, and combination therapy is our best hope for durable outcome and satisfied patients. RP
| Albert J. Augustin, MD, is on the faculty of ophthalmology at Klinikum Karlsruhe in Karlsruhe, Germany. The author does not report any financial interest in the therapies discussed, although he has been paid as a consultant to QLT Inc. Dr. Augustin can be reached at 106020.560@compuserve.com. |
REFERENCES
- Friedman DS, O'Colmain BJ, Munoz B, et al. Prevalence of age-related macular degeneration in the United States. Arch Ophthalmol. 2004;122:564-572.
- Klein R, Klein BE, Knudtson MD, et al. Fifteen-year cumulative incidence of age-related macular degeneration: the Beaver Dam Eye Study. Ophthalmology. 2007;114:253-262.
- Varma R, Fraser-Bell S, Tan S, et al; Los Angeles Latino Eye Study Group. Prevalence of age-related macular degeneration in Latinos: the Los Angeles Latino eye study. Ophthalmology. 2004;111:1288-1297.
- Munoz B, Klein R, Rodriguez J, et al. Prevalence of age-related macular degeneration in a population-based sample of Hispanic people in Arizona: Proyecto VER. Arch Ophthalmol. 2005;123:1575-1580.
- Narayanan R, Butani V, Boyer DS, et al. Complement factor H polymorphism in age-related macular degeneration. Ophthalmology. 2007;114:1327-1331.
- Shastry BS. Assessment of the contribution of the LOC387715 gene polymorphism in a family with exudative age-related macular degeneration and heterozygous CFH variant (Y402H). J Hum Genet. 2007;52:384-387.
- Moshfeghi DM, Blumenkranz MS. Role of genetic factors and inflammation in age-related macular degeneration. Retina. 2007;27:269-275.
- Shuler RK Jr, Hauser MA, Caldwell J, et al. Neovascular age-related macular degeneration and its association with LOC387715 and complement factor H polymorphism. Arch Ophthalmol. 2007;125:63-67.
- Kaiser PK. Verteporfin photodynamic therapy and anti-angiogenic drugs: potential for combination therapy in exudative age-related macular degeneration. Curr Med Res Opin. 2007;23:477-487.
- Augustin AJ, Offermann I. Emerging drugs for age-related macular degeneration. Expert Opin Emerg Drugs. 2006;11:725-740.
- Augustin AJ, Puls S, Offermann I. Triple therapy for choroidal neovascularization due to age-related macular degeneration: Verteporfin PDT, bevacizumab, and dexamethasone. Retina. 2007;27:133-140.
- Spaide RF. Rationale for combination therapies for choroidal neovascularization. Am J Ophthalmol. 2006;141:149-156.
- Kaiser PK. Verteporfin therapy in combination with triamcinolone: published studies investigating a potential synergistic effect. Curr Med Res Opin. 2005; 21:705-713.
- Augustin AJ, Schmidt-Erfurth U. Verteporfin therapy and triamcinolone acetonide: convergent modes of action for treatment of neovascular age-related macular degeneration. Eur J Ophthalmol. 2006;16:824-834.
- Schmidt-Erfurth U, Gabel P, Hohman T; Protect Study Group. Preliminary results from an open-label, multicenter, phase II study assessing the effects of sameday administration of ranibizumab (Lucentis™) and verteporfin PDT (PROTECT Study). Paper presented at: Annual Meeting of the Association for Research in Vision and Ophthalmology; April 30-May 4, 2006; Fort Lauderdale, FL.
- Funk M, Michels S, Wagner J, et al. Vascular effects of combined ranibizumab (Lucentis®) and verteporfin (Visudyne®) therapy in patients with neovascular age-related macular degeneration. Paper presented at: Annual Meeting of the Association for Research in Vision and Ophthalmology; April 30-May 4, 2006; Fort Lauderdale, FL.
- Wagner J, Simader C, Kiss C, et al. Changes in functional macular mapping in patients with neovascular age-related macular degeneration receiving combination of verteporfin (Visudyne®) and ranibizumab (Lucentis™) therapy. Paper presented at: Annual Meeting of the Association for Research in Vision and Ophthalmology; April 30-May 4, 2006; Fort Lauderdale, FL.
- Colina-Luquez JM, Liggett PE, Tom D, et al. Prospective and preliminary study evaluating triple therapy of intravitreal triamcinolone, photodynamic therapy and pegaptanib sodium for choroidal neovascularization. Paper presented at: Annual Meeting of the Association for Research in Vision and Ophthalmology; April 30-May 4, 2006; Fort Lauderdale, FL.
- Offermann I, Altinay A, Schmidt-Erfurth U, et al. Intravitreal bevacizumab for the treatment of remaining choroidal neovascularization (CNV) activity following combination therapy (PDT and triamcinolone). Paper presented at: Annual Meeting of the Association for Research in Vision and Ophthalmology; April 30-May 4, 2006; Fort Lauderdale, FL.