







ICG Dye Is Back in Our Armamentarium
DAVID M. BROWN, MD, FACS • MATHEW S. BENZ, MD
Finally, indocyanine green (ICG) dye is back in the clinic and the operating theater! Most of us didn't realize how important ICG dye was to our daily practice until Akorn pharmaceuticals (Buffalo Grove, IL), the sole North American supplier of ICG dye, temporarily could not supply the dye for the majority of 2007. ICG has a strong affinity to proteins both in plasma (it is FDA-approved indication for angiography) and to basement membranes (extremely helpful to stain the internal limiting membrane in macular surgery).
ICG ANGIOGRAPHY IS CRITICAL FOR IMAGING CHOROIDAL PATHOLOGY
Fluorescein angiography (FA) is an important diagnostic tool for the retinal specialist, but the introduction of optical coherence tomography (OCT) has fueled arguments over the possible obsolescence of FA. Lost in this discussion has been the advances made using indocyanine green angiography (ICGA), which, when combined with recent advances in imaging technology, has enabled views of the choroidal circulation unobtainable by either OCT or FA.1 ICGA enables analysis of the choroidal circulation and interaction with the retina in contrast to FA, which primarily is focused on the retinal vasculature lying above the darkened background of the retinal pigmented epithelium (RPE).
ICGA can be performed with film and digital fundus cameras that have been modified with an assortment of filters to excite and detect ICG. However, in our experience, ICG angiography is most useful when acquired with a confocal scanning laser ophthalmoscope (cSLO). Modified traditional fundus cameras cannot produce as intense an infrared light illumination and do not have the same sensitivity to selectively detect the returning fluorescent signal. The confocal principle of blocking stray, out-of-focus light and the use of peak wavelength laser light sources makes the cSLO superior in capturing ICG angiographic images. In addition, the high-speed nature of laser imaging enables videography of the dye uptake, yielding a different diagnostic dimension than still images alone.
| David M. Brown, MD, FACS and Matthew Benz, MD are principals at Vitreoretinal Consultants in Houston, TX. Their research and clinical interests are focused on diseases of the macula including macular surgery, age related macular degeneration, diabetic retinopathy and retinal angiogenesis. |
ICG is a larger molecule than fluorescein and has a high binding affinity to plasma proteins, reducing its diffusion though choriocapillary fenestrations. In addition, ICG is excited and fluoresces under near infrared light, which easily penetrates the RPE, in contrast to fluorescein, which is excited by shorter-wavelength visible light (488 nm) and is absorbed (blocked) by the RPE. So, slower diffusion to the retina, combined with infrared transparency of the RPE, allows ICG to light up the underlying choroidal vasculature when fluorescein cannot. This is particularly important in the diagnosis of choroidal disorders such as retinal angiomatous proliferation (RAP) lesions in neovascular AMD, diseases of increased choroidal vessel permeability (central serous retinopathy and idiopathic polypoidal choroidopathy), and inflammatory diseases of the choroid like multiple evanescent white dot syndrome (MEWDS) and birdshot choroidopathy.
IDENTIFICATION OF RAP LESIONS
One of the most dramatic examples of choroidal circulatory imaging has been the crisp identification of chorioretinal anastomoses, also referred to as retinal angiomatous proliferation or RAP. Originally believed to be present in a minority of choroidal neovascular AMD cases, current literature is showing rates of up to 20%.2 Cases with RAP lesions are often more refractive to all types of therapy than CNV without them. RAP lesions are easy to document through simultaneous FFA and ICG angiography, which can be performed with cSLO ICG angiography (Figure 1).
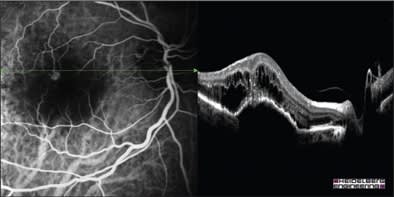
Figure 1 Courtesy of Heidelberg Engineering Inc.
Figure 1. Simulataneous ICG/FA left and Spectralis (Heidelberg Engineering, Inc.) OCT right show intraretinal location characteristics of RAP.
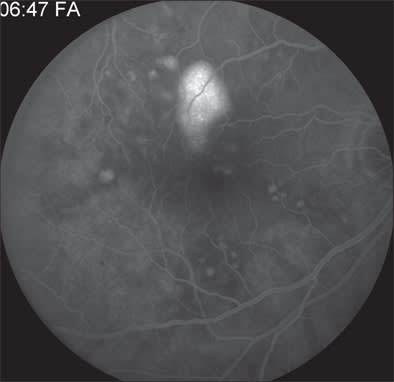
Figure 2A. Late-phase angiogram showing filling of pigment epithelium detachment in chronic CSR.
CENTRAL SEROUS RETINOPATHY
Fluorescein angiography often documents pinpoint areas of hyperflourescence in central serous retinopathy (CSR) and clearly both FFA and OCT show the resulting pigment epithelial detachments (Figures 2A and 2B). However, ICGA documents marked choroidal hyperpermeability that persists even after the fluorescein leakage resolves. Figure 2C demonstrates the marked engorgement and leakage of the choroidal vessels along with their correlation to the retinal vessels in this same patient and Figure 2D (a widefield mid-phase cSLO ICG image) demonstrates that this choroidal hyperpermeability exists throughout the choroidal circulation and is multifocal, existing even outside the arcades. Patients with hyperpermeable choroidal vessels often have frequent and severe CSR recurrences and may possibly be predisposed to the development of polypoidal choroidal vasculopathy (PCV).
POLYPOIDAL CHOROIDAL VASCULOPATHY
Polypoidal choroidal vasculopathy presents with multiple recurrent serosanguinous detachments of the RPE and neurosensory retina secondary to leakage and bleeding from choroidal vascular lesions (Figure 3A). Yanuzzi and associates describe the characteristic ICG angiographic findings of polypoidal lesions in the choroidal circulation and branching vascular networks (Figure 3B). ICGA can also show increased vascular permeability of the choroidal vasculature that can be indicative of a poorer prognosis.
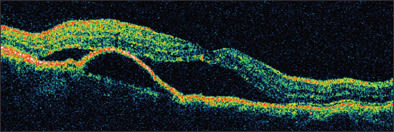
Figure 2B. OCT reveals pigment epithelium detachment as well a serous retinal detachment involving the fovea.
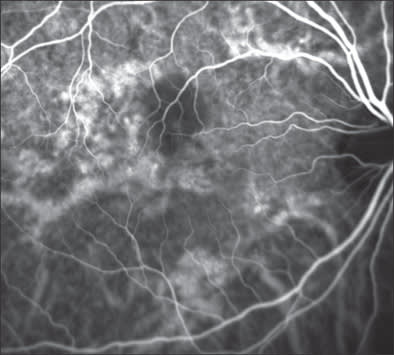
Figure 2C. Marked engorgement and hyperpermeability of choroidal vessels seen in this early ICG phase.
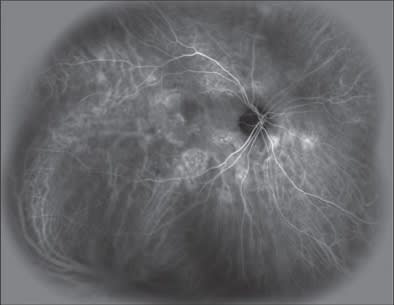
Figure Images 2-5 by Eric N. Kegley, CRA, COA of Vitreoretinal Consultants.
Figure 2D. Wide field automatic real-time ICG shows involvement of central serous retinopathy in both the posterior pole and lesions nasal to the nerve.
MEWDS
Inflammatory disorders of the choroids such as MEWDS are often very difficult to diagnose. The clinical findings are often subtle (Figure 4A) and FFA does not identify the pathology in many cases (Figure 4B). The ICG findings, however, are usually very striking with multiple areas of choroidal hypoperfusion, often throughout the posterior pole (Figure 4C).
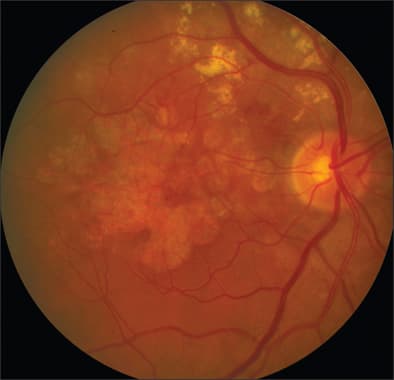
Figure 3A. Color image reveals hemorrhaging and hard exudates along superior arcade extending in the macula in a patient with polypoidal choroidal vasculopathy.
CHOROIDAL HYPOPERFUSION FROM PHOTODYNAMIC THERAPY
Standard fluence verteporfin photodynamic therapy (PDT) causes choroidal hypoperfusion, which is easily documented by ICGA. This can be helpful to titrate fluence of repeat PDT when used in combination therapy with an anti-VEGF therapy. While mild choroidal hypoperfusion may not be harmful to ultimate VA, those patients with profound VA loss typically have profound choroidal ischemia. Figures 5A-5C demonstrate an early, mid, and late phase ICG 1 week after 40% fluence verteporfin PDT treatment in combination with intravitreal ranibizumab. This particular patient had persistent choroidal hypoperfusion up to 6 months following PDT treatment but maintained 20/25 VA.
CONTRASTING ICGA WITH FA
So what does ICGA add to our diagnostic capabilities? For diseases that are primarily choroidal, they allow us to make more definite diagnosis and initiate and manage treatment decisions. ICG can often provide a clear answer where other diagnostics are either negative, not clear, or are in conflict with each other. We "made do" in the 8 months that ICG dye was unavailable but I felt like Tiger Woods without any wedges. Yes, Tiger can use a partial swing with a 9 iron and still win a few tournaments, but it's definitely a handicap.
INDOCYANINE GREEN IN VITRECTOMY
The use of ICG as a surgical adjunct to pars plana vitrectomy has been widely reported and was "standard of care" in our treatment of macular holes and many other macular surgery cases before the ICG shortage.3-5 The most common indication for the use of ICG is to stain the internal limiting membrane (ILM) during pars plana vitrectomy, facilitating its visualization and subsequent removal in surgical procedures involving macular pathology, such as macular hole, epimacular membrane, vitreomacular traction syndrome, and diabetic macular edema.
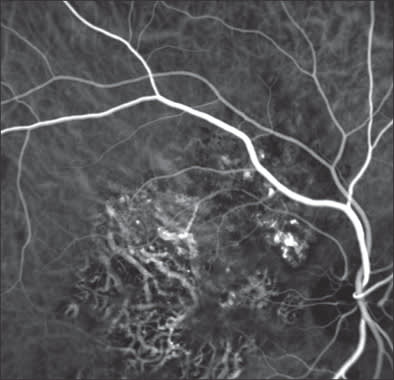
Figure 3B. Early-frame ICG reveals characteristic polypoidal lesions in superonasal macula.
Without question, staining the ILM with ICG facilitates a challenging surgical maneuver. Multiple prior reports have questioned the relative safety of ICG staining of the ILM, proposing multiple potential causes for so-called ICG toxicity.6-9 Other reports have indicated an improved surgical anatomic success rate, in particular for macular hole surgery, in patients who undergo removal of the ILM during vitrectomy.10-12 Recently, after manufacturing concerns related to the main commercial supplier of ICG were raised by the FDA, a prolonged time period passed with no easy availability of ICG in the United States. Although these concerns have passed and ICG is readily commercially available again, the previous time period without ICG caused us to adjust some of our surgical approaches and reassess our use of ICG in macular surgical procedures.
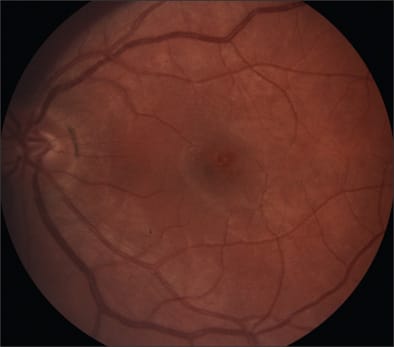
Figure 4A. Evanescent legions with some granularity of the fovea in a patient with classic MEWDs.
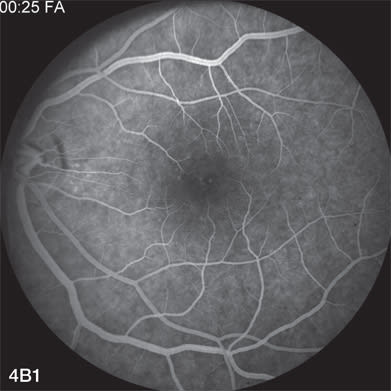
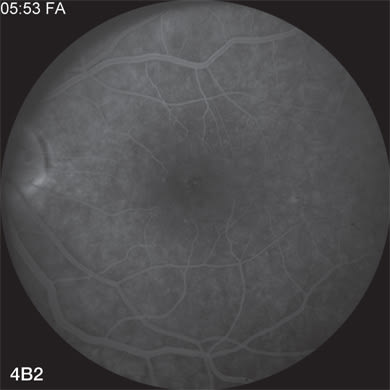
Figure 4 B. FA early and late shows only subtle changes corresponding to the retinal legions.
ICG is typically applied to the surface of the ILM after separation of the posterior hyaloid and removal of the cortical vitreous. Surgeons may use varying concentrations and time exposures when applying ICG to the ILM. Some surgeons prefer to perform a partial fluid-air exchange prior to applying ICG, while others apply ICG directly over the macula under fluid. In addition, devices have been described to more selectively apply ICG to intact ILM and minimize direct exposure of the RPE to ICG.13
Once ICG has been used to stain the surface of the ILM, an edge of the ILM must be lifted and then peeled at an angle tangential to the macular surface. Different techniques may be used to lift the ILM and create a surgical plane between the ILM and underlying tissue. A bent or straight microvitreoretinal (MVR) blade, a barbed needle, or a Tano brush may be used to lift an edge of the ILM. Alternatively, forceps may be used to directly grasp, pinch, and lift the ILM and then to proceed with peeling the ILM. We have found increasing comfort with using forceps for this maneuver as the manufacture of fine vitreoretinal forceps has improved. In particular, we have found the new disposable Alcon (Fort Worth, TX) 23-g ILM forceps to have improved tip architecture, facilitating direct grasping of the ILM.
Visualization of the ILM without ICG staining is certainly possible, but challenging. During the time when we did not have ready access to ICG for our surgical procedures, we tried several alternatives, including triamcinolone acetonide and Trypan blue (anterior segment concentration). Although variably effective at times, neither of these options was as good at staining the ILM as ICG. We also peeled ILM (or at least attempted to peel ILM) without the aid of an ILM stain. In our experience, we were rarely as confident in our ability to remove the ILM as completely as we desired without the use of ICG. Nevertheless, the large majority of our macular holes closed after surgical intervention and our patients seemed to do well. Although we have not done a thorough retrospective review of our cases, the time period without access to ICG may contain useful data. Several prior reports have indicated similar visual outcomes in macular hole surgery with or without ILM peeling.10-12 Using ICG in macular hole surgery may involve inherent trade-offs. Greater visualization of the ILM with ICG may facilitate its removal, but possible toxicity issues may mitigate visual gains. On the other hand, attempting to peel ILM without the use of ICG may lead to a greater risk of surgical trauma to the macula.
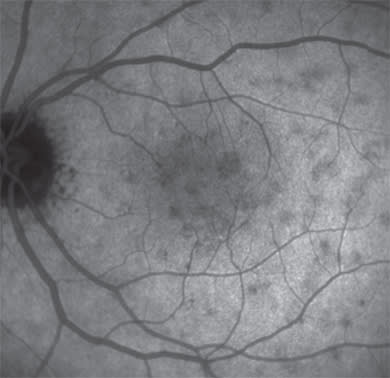
Figure 4C. Very late-frame ICG reveals multiple areas of involvement that are pathogneumonic for MEWDS.
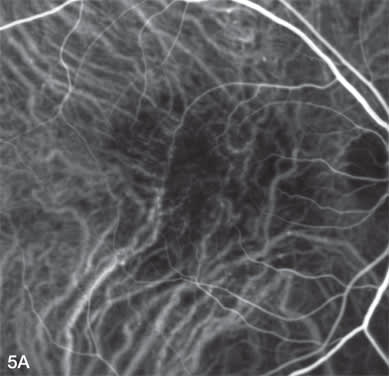
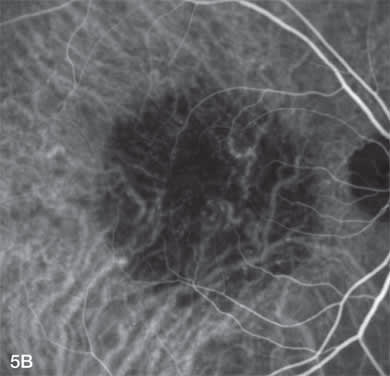
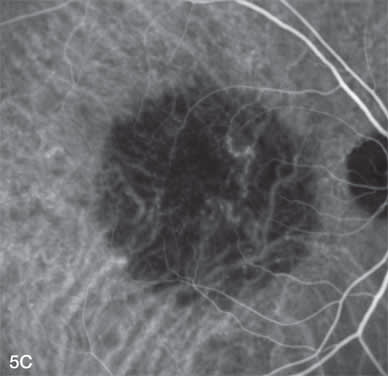
Figure 5A, B, and C. Early, mid, and late-phase ICG demonstrate marked choroidal hypoperfusion one week after reduced fluence verteporfin photodynamic therapy.
The potential mechanisms of toxicity of ICG are varied and somewhat controversial. Possible mechanisms may include direct injury to retinal cells, light toxicity induced by the application of ICG, direct damage to the RPE, apoptosis in RPE cells, an osmolarity effect of ICG, amongst other possibilities. Perhaps the most widely reported possible mechanism of ICG toxicity is damage to the RPE. Several reports have demonstrated this possibility, both clinically as well as in the laboratory.7,8,14-16 It would certainly make sense to minimize direct exposure of the RPE to ICG and care should be taken to decrease the exposure time in macular hole cases in particular.
Another widely reported possible cause of toxicity is related to light exposure. In order to understand why this may be an issue with ICG, one needs to understand the light absorption properties of ICG. The peak of the light absorption spectrum of protein-bound ICG is around 810 nm.17 Histologic analysis has revealed that ICG molecules used to stain ILM are mainly bound to extracellular matrix proteins like type IV collagen.18 Thus, ICG binding to ILM likely decreases polymer formation and shifts the absorption toward 810 nm. This is roughly the same wavelength emitted by a diode laser. Hence the multiple reports that have evaluated using ICG as an adjunct to diode laser procedures.19,20 These same properties that may be useful in one sense could be harmful in another. If the light source used during a vitrectomy contains the 810 nm wavelength and exposure time is long, the possibility of light toxicity could exist.
Once ICG became readily available once again, we returned to using it for many of our cases when we want to peel ILM. We try to limit exposure and potential toxicity issues by using a dilute solution of ICG, avoiding reapplication of ICG, and limiting surgical time and light exposure.
Macular surgery can be performed with or without the use of surgical adjuncts such as ICG. Although our recent experiences without access to ICG reminded us that we can achieve successful outcomes in macular surgery without the use of ICG, we are happy to have it available once again to assist us in those cases where we deem it necessary. RP
REFERENCES
- Stanga PE, Lim JI, Hamilton; Indocyanine green angiography in chorioretinal diseases: indications and interpretations: an evidence-based update. Ophthalmology. 2003;110:15-21.
- Massacesi AL, Sacchi L, Bergamini F, Bottoni F. The prevalence of retinal angiomatous proliferation in age-related macular degeneration with occult choroidal neovascularization, Graefes Arch Clin Exp Ophthalmol. 2008;246:89-92. [Epub 2007 Jul 25.]
- Kadonosono K, Itoh N, Uchio E, et al. Staining of the internal limiting membrane in macular hole surgery. Arch Ophthalmol. 2000;118:1116-1118.
- Da Mata AP, Burk SE, Riemann CD, et al. Indocyanine green-assisted peeling of the retinal internal limiting membrane during vitrectomy surgery for macular hole repair. Ophthalmology. 2001;108:1187-1192.
- Gandorfer A, Messmer EM, Ulbig MW, et al. Indocyanine green selectively stains the internal limiting membrane. Am J Ophthalmol. 2001;131:387-388.
- Kanda S, Uemura A, Yamashita T, et al. Visual field defects after intravitreous administration of indocyanine green in macular hole surgery. Arch Ophthalmol. 2004;122:1447-1451.
- Maia M, Haller JA, Pieramici DJ, et al. Retinal pigment epithelial abnormalities after internal limiting membrane peeling guided by indocyanine green staining. Retina. 2004;24:157-160.
- Engelbrecht NE, Freeman J, Sternberg P, et al. Retinal pigment epithelial changes after macular hole surgery with indocyanine green-assisted internal limiting membrane peeling. Am J Ophthalmol. 2002;133:89-94.
- Sakamoto T, Itaya K, Noda Y, Ishibashi T. Retinal pigment epithelial changes after indocyanine green-assisted vitrectomy. Retina. 2002;22:794-796.
- Sheidow TG, Blinder KJ, Holekamp N, et al. Outcome results in macular hole surgery: an evaluation of internal limiting membrane peeling with and without indocyanine green. Ophthalmology. 2003;110:1697-1701.
- Gass CA, Hartiglou C, Schaumberger M, Kampik A. Functional outcome of macular hole surgery with and without indocyanine green-assisted peeling of the internal limiting membrane. Graefes Arch Clin Exp Ophthalmol. 2003;241:716-720.
- Ando F, Sasano K, Ohba N, et al. Anatomic and visual outcomes after indocyanine green-assisted peeling of the retinal internal limiting membrane in idiopathic macular hole surgery. Am J Ophthalmol. 2004;137:744-746.
- Meyer CH, Rodrigues EB. A novel applicator for the selective painting of pre-retinal structures during vitreoretinal surgery. Graefes Arch Clin Exp Ophthalmol. 2005;243:487-489.
- Sippy BD, Engelbrecht NE, Hubbard GB, et al. Indocyanine green effect on cultured human retinal pigment epithelial cells: implication for macular hole surgery. Am J Ophthalmol. 2001;132:433-435.
- Ikagawa H, Yoneda M, Iwaki M, et al. Chemical toxicity of indocyanine green damages retinal pigment epithelium. Invest Ophthalmol Vis Sci. 2005;46:2531-2539.
- Rezai KA, Farrokh-Siar L, Ernest JT, van Seventer GA. Indocyanine green induces apoptosis in human retinal pigment epithelial cells. Am J Ophthalmol. 2004;137:931-933.
- Landsman MLJ, Kwant G, Mook GA, Zijlstra WG. Light-absorbing properties, stability and spectral stabilization of indocyanine green. J Appl Physiol. 1976;40:575-583.
- Kwok AK, Li WW, Pang CP, et al. Indocyanine green staining and removal of internal limiting membrane in macular hole surgery: histology and outcome. Am J Ophthalmol. 2001;132:178-183.
- Reichel E, Puliafito CA, Duker J, Guyer D. Indocyanine green dye enhanced diode photocoagulation of poorly defined subfoveal choroidal neovascularization. Ophthalmic Surg. 1994;25:195-201.
- Costa RA, Farah ME, Cardillo JA, Belfort R Jr. Photodynamic therapy with indocyanine green for occult subfoveal choroidal neovascularization caused by age-related macular degeneration. Curr Eye Res. 2001;23:271-275.