







Photo Essay: Recurrent Toxoplasma Chorioretinitis With Kyrieleis' Vasculitis
ANNE E. FUNG, MD · DAVID HEIDEN, MD · SARAH HUGGANS · DENICE BARSNESS
A 39-year-old native of Russia presented for an urgent-care appointment with complaints of floaters in the left eye, worsening over 3 weeks. On presentation, visual acuity (VA) was 20/25 OS with intraocular pressure of 13 mm Hg. The anterior segment was quiet, but 2 to 3+ vitreous cells were present (Figures 1 to 3).
A 1-month course of trimethoprim 160 mg/sulfa-methoxazole 800 mg double strength (DS) bid was given. The infection and inflammation decreased over 2 months and coalesced into a yellow chorioretinal scar (Figures 4 and 5). Seven weeks after the last follow-up, the patient noticed blurred vision and was found to have a Kyrieleis' pattern of inflammation. VA was 20/40. She was restarted on trimethoprim/sulfamethoxazole DS for 6 weeks. Kyrieleis first described this beaded pattern of vascular inflammation in 1933. It is predominantly associated with toxoplasma infection but has been seen in syphilis, tuberculosis, and herpes zoster retinopathy.1,2 RP

Figure 1. Montage FA of a typical primary toxoplasma chorioretinitis – The infection blocks fluorescence centrally with hyperfluorescence present at the edges of the lesion. The infection has also reduced perfusion in the arteriole distally and generalized venous leakage consistent with vasculitis is present. Mild vitreous cells blur the image.
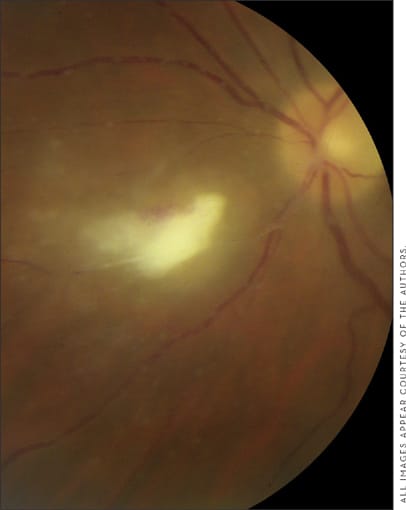
Figure 2. Primary toxoplasma chorioretinitis.

Figure 3. Primary toxoplasma chorioretinitis montage fundus photo. White chorioretinitis inferotemporal to the optic nerve, vasculitis and blurring of image from vitreous cells is present.
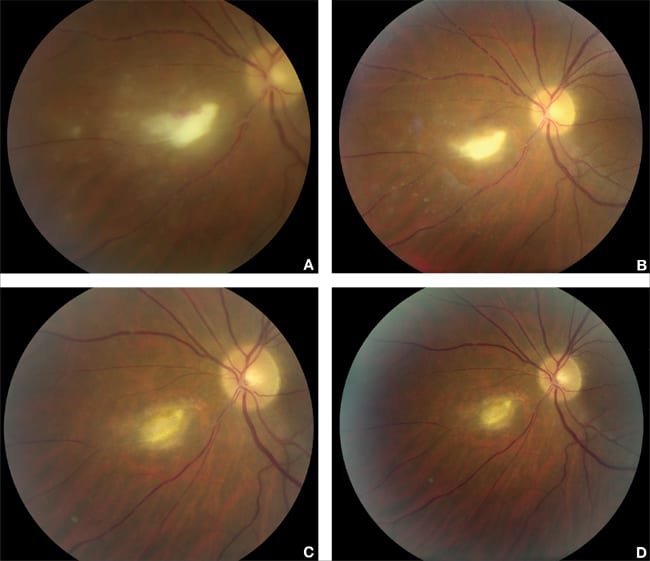
Figure 4. Resolution of toxoplasma chorioretinitis during and following treatment with oral trimethoprim. A-D Images 1-5 weeks following initiation of therapy showing decreasing inflammation and gradual coalescence to an inactive scar.
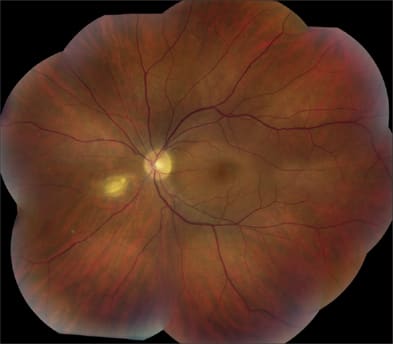
Figure 5. Montage of quiescent toxoplasma scar before recurrence.
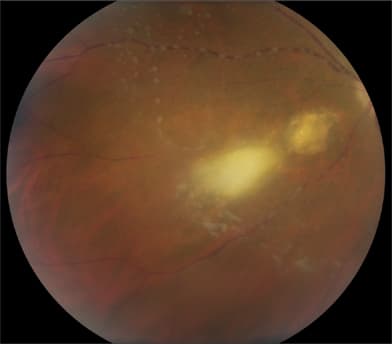
Figure 6. Magnification of recurrent toxoplasma infection distal to original site. Kyrieleis' pattern of arteritis is present as yellowish plaques within the artery that appear nodular and do not extend outside the vessel.
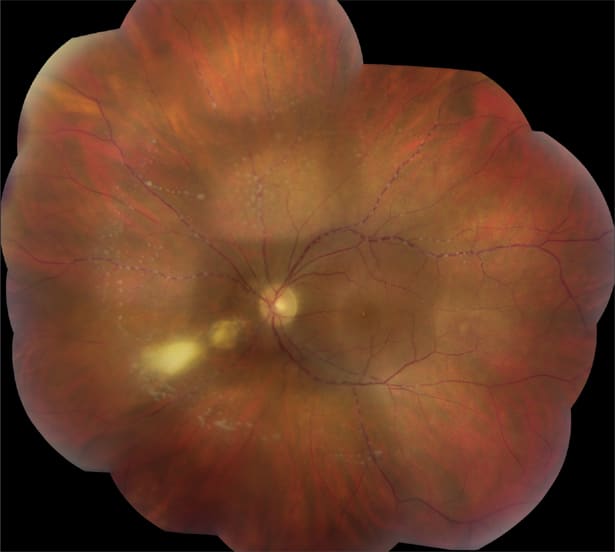
Figure 7. Montage photo of recurrent toxoplasma infection with Kyrieleis' vascular plaques throughout the fundus.
| Anne E. Fung, MD, is a medical retina specialist and David Heiden, MD, is a uveitis specialist with Pacific Eye Associates. Sarah Huggans is a certified photographer and Denice Barsness is the director of ophthalmic imaging with the Ophthalmic Diagnostic Center at the California Pacific Medical Center The authors have no financial disclosures to make. Dr. Fung can be reached via e-mail at annefungmd@yahoo.com. |
REFERENCES
- Bisighini SL, Pagliuso LM. Retinal vasculitis: a diagnostic dilemma. Clin Eye Vis Care. 1997;9:71-84.
- Jain IS, Singh K. Segmental arteritis. Indian J Ophthalmol. 1966;14:229-223.