







Combination Instrument Enhances Patient Care
A Duke University physician describes his experience with multi-modality imaging.

BY SCOTT W. COUSINS, MD
As Dr. Kaiser explained in the previous article, spectral domain optical coherence tomography (OCT) is the future of this technology. All of the newest instruments are based on spectral domain, rather than time domain, processes. Therefore, they all collect more data faster and, as a result, produce higher resolution images. Some of the instruments combine other imaging modalities with spectral domain OCT.
In our practice, we have been using the Spectralis HRA+OCT from Heidelberg Engineering, which combines high resolution cross-sectional images of the retina with 4 imaging modalities: infrared, fluorescein angiography, indo-cyanine green (ICG) angiography or autofluorescence. Having all of these modalities in one device allows us to apply them in new ways and improve patient care.
INFRARED
Infrared imaging is, of course, a good modality for visualizing surface abnormalities such as epiretinal membranes. With the use of a pseudo-color component with the Spectralis HRA+OCT the infrared images are almost good enough to project as fundus photos.
FLUORESCEIN ANGIOGRAPHY
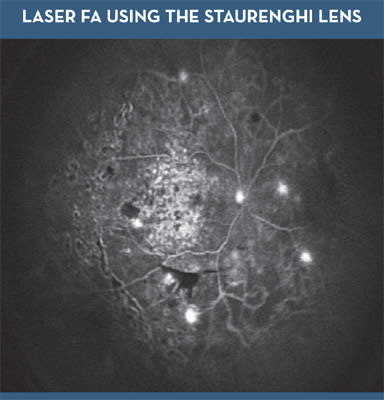
Spectralis HRA+OCT is also an outstanding fluorescein angiography unit. It uses laser excitation to provide dynamic high-speed movies with sharp resolution. I find it useful to be able to register the OCT scans with angiography. For example, simply moving the cursor over diabetic microaneurysms shows their location in relation to the fovea for the purpose of delivering focal laser treatment.
The device has wide field capability as well. A 55-degree field of view can be obtained without contact, and a contact Staurenghi lens (Figure 1) provides a complete wide field view. We have clinical evidence to suggest that diabetic macular edema patients with severe peripheral nonperfusion may be most susceptible to treatment with anti-vascular endothelial growth factor (VEGF) therapy, so that wide field imaging of patients with DME will be increasingly useful.
ICG ANGIOGRAPHY
ICG angiography with the Spectralis HRA+OCT is fundamentally different than with standard flash technology. As it does with fluorescein angiography, the Spectralis acquires dynamic, high-speed movies (up to 16 frames per second) for ICG imaging.
Most of the important information occurs in the first 15 or 20 seconds of these videos. Essentially, we have to learn to read these dynamic ICG angiograms just like we learned to read fluoresceins in our fellowships. The studies image choroidal neovascularization (CNV) through three phases: an arterial phase, a capillary phase and a venous phase. What we have learned with this instrument contradicts the conventional wisdom of CNV morphology that we surmised from fluorescein angiography. The conventional wisdom suggests that CNV are capillaries derived from capillaries. In reality, most CNV lesions are a vascular complex with a feeding artery, a capillary unit and a draining vein. This is important knowledge because it allows us to classify lesions into categories based on whether they are perfused by tiny thread-like feeder vessels or large branching arteries. Those CNV perfused by small feeders with low flow capillaries appear to respond well to anti-VEGF therapy. On the other hand, CNV perfused by large feeders with many branching arteriolar vascular complexes are high flow and respond well to photodynamic therapy (PDT).

FIG. 2: MANY CLASSIC CNV DEMONSTRATE WELL DEFINED VASCULAR COMPLEXES
I have used ICG angiography with the Spectralis HRA+OCT in many cases to enhance patient care. For example, since my fellowship, I had always been fascinated by a comment made by J. Donald M. Gass, MD. He said that all serous pigment epithelial detachments (PEDs) are vascularized. Others disagreed, maintaining that serous PEDs are manifestations of dry age-related macular degeneration, caused from fluid that cannot pass through the lipid filled Bruch's membrane. Recently one of my patients presented with acute vision loss after carotid artery surgery associated with a notched PED and subretinal fluid. Fluorescein angiography showed nothing in the PED notch. However, high-speed ICG angiography showed a prominent feeder artery and a capillary complex. The patient actually had a vascularized PED. We have imaged a series of 55 consecutive PEDs with ICG and found about half of them to have neovascularization that was not evident with fluorescein. We are now treating those patients.
As I mentioned, it appears the degree of arteriolar vascularization in CNV is indicative of which patients will respond to anti-VEGF therapy. In my hands 15% to 20% of CNV cases fail to respond anatomically to anti-VEGF therapy, and some lesions enlarge or bleed while on therapy. I have found that in patients who are doing well on anti-VEGF therapy, ICG angiography with the Spectralis shows the capillary portion of the CNV decreases or disappears over time. Conversely, in someone who is not doing well or fails to respond, ICG angiography usually shows an arteriolarized CNV with large branching arterioles and enlargement of the capillary portion. In one of my patients, who was needing monthly therapy, ICG angiography revealed a large feeder vessel. The leakage was not only VEGF-driven but flow-driven as well.
In a similar case, one of my patients was not responding to treatment with bevacizumab (Avastin, Genentech). Based on ICG imaging, I treated the feeder complex, not the entire capillary complex. His retinal thickness normalized and the eye remained dry for 9 months. Cases like these leave no doubt in my mind ICG-directed PDT is a very useful aspect of this instrument.
AUTOFLUORESCENCE
I have been using fundus autofluorescence for the past two years and have concluded it is an underappreciated technology. With other instruments, fundus autofluorescence requires acquisition of a single image with bright flash illumination and a specific filter set. The problem with this approach is that the images have low contrast. With the Spectralis HRA+OCT, however, the unit uses laser illumination and can average 15 images to enhance the contrast.
Similar to other autofluorescence instruments, the Spectralis measures retinal lipofuscin, which is the byproduct of retinal pigment epithelium phagocytosis that accumulates as particles within cells. It appears to be derived from vitamin A metabolism. In fact, Sirion Therapeutics is currently evaluating the drug fenretinide as a way to block vitamin A transport to prevent lipofuscin buildup and therefore prevent geographic atrophy (GA) progression. Several other drugs are on their way to clinical trials for GA, so this is a condition that will become a high priority for reseach and clinical care. Most pharmaceutical companies setting up GA clinical trials are choosing the Spectralis HRA+OCT as their standard instrument.
Autofluorescence also will be useful in unusual maculopathies. I recently obtained a fluorescein angiogram using the Spectralis HRA+OCT in a patient with Stargardt's disease. In addition, lypofuscin and A2E hyperfluoresced in autofluorescence mode. What I found very informative is that I also was able to align the cursor at the margins of the area of atrophy and scrutinize the structure of the retina (Figure 4). In this case, disruption of the outer segments was evident. Suspecting that progressive vision loss would occur in this case, we began counseling the patient about low vision services and occupational planning.
I believe the images we can obtain and correlate using the Spectralis HRA+OCT also will teach us more about how to interpret structure/function relationships. For example, one of our hypotheses, put forth by Alan C. Bird, MD, is that intact autofluorescence in the retina overlying CNV indicates eyes that have good visual potential, and absent autofluorescence over CNV suggests poor vision potential.
FIVE WAYS TO IMAGE ARE BETTER THAN ONE
Now that we have been using the Spectralis HRA+OCT in practice, we have experienced many cases to illustrate that we cannot appreciate what we cannot see. For example, in one patient, we had been using time domain OCT to follow a tiny amount of fluid in one eye of a patient who had a disciform scar in the other eye. He was not sure whether he wanted to consent to anti-VEGF therapy, so we imaged the retina with the Spectralis HRA+OCT. This gave us the advantage of scanning the entire macula rather than only six cuts through the fovea. What we found was extensive fluid outside of the fovea, including along the superior and juxtafoveal zones. Zones of his contained fluid that had not been detected with time domain technology. Because this new instrument allows us to look at a volumetric OCT scan and also evaluate a dynamic video of the same area, we get a better appreciation for the extent and severity of pathology.

FIG. 3
Based on my experience so far, the multiple imaging modalities of the Spectralis HRA+OCT give us the ability to learn more about the pathology of each individual eye. That ability adds a great deal more value for our practices than the spectral domain OCT component alone.
| Scott W. Cousins, MD, is director of the Duke Center for Macular Diseases at the Duke University Eye Center in Durham, N.C. He can be reached at scott.cousins@duke.edu or (919) 684-3090. |