







feature
Transpupillary
Thermotherapy for Age-Related Macular Degeneration
FAREED
ALI, MD, FRCS(C)
|
|
|
Figure 1. Red-free photo at initial presentation. |
CLINICAL HISTORY AND DIAGNOSTIC EVALUATION
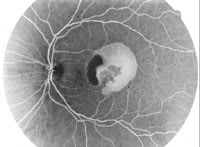
A white female patient, 68 years of age, presented with a 3-week history of sudden onset of decrease in vision in her left eye with progressive deterioration. On presentation her vision was 20/30 OD and 20/400 OS. The right eye had dry age-related macular degeneration (AMD). The left eye had thick subretinal blood in the center of the macula with diffuse retinal edema and a visible subfoveal vascular membrane (Figure 1). Fluorescein angiography showed significant blockage due to subretinal blood with a small area of poorly-defined late leakage under the fovea (Figure 2). Optical coherence tomography (OCT) showed significant diffuse subretinal fluid and retinal edema (Figure 3). A diagnosis of an occult subretinal neovascular membrane in her left eye due to exudative AMD was made.
Treatment options were discussed with the patient. It was explained that without any treatment, a 70% chance of progressive and significant vision loss existed. At the time of presentation, anti-VEGF therapies were not available. Additionally, photodynamic therapy (PDT) with verteporfin (Visudyne, Novartis) was an uninsured service for occult membranes and the patient was unwilling and unable to pay for the cost of this therapy. Transpupillary thermotherapy (TTT) was discussed with the patient. It was explained that TTT had a 75% chance of preventing further significant visual loss, a 10% chance of noticeable vision improvement, and required only a single treatment in 80% of patients. The patient agreed to treatment with TTT.
|
|
| Figure 2. Late-phase fluorescein angiogram at initial presentation. |

TREATMENT
Transpupillary thermotherapy was performed using a slit-lamp delivered 810-nm diode laser (model SLx, IRIDEX, Mountain View, Calif). A 3.0-mm laser spot size setting was used delivered through a 1.05-magnification laser contact lens. A power setting of 780 mW and treatment duration of 60 seconds was used. The patient reported only a mild warmth sensation during treatment and there was no visible color change in the retina observed during the therapy. The patient returned for routine follow-up visits during the next several weeks.
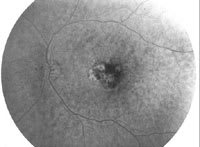
At the 3-month post-TTT visit, the vision in the patient's left eye had improved to 20/60. There was a significant reduction in subretinal blood and retinal edema (Figure 4). Fluorescein angiogram showed resolution of subretinal blood with mild subretinal late staining only (Figure 5). OCT showed significant reduction in subretinal fluid and retinal edema (Figure 6).
DISCUSSION
|
|
|
Figure 3. OCT at initial presentation. |

This case study describes effective treatment of an occult subretinal membrane due to exudative AMD. The patient was treated using standard laser parameters for the specific lesion and patient characteristics. Minor changes in laser treatment parameters are sometimes required for lesions of different size and for variations in retinal pigmentation due to racial variations. It should be noted that this patient presented prior to the availability of any anti-VEGF therapies such as pegaptanib sodium (Macugen, OSI), bevacizumab (Avastin, Genentech), and ranibizumab (Lucentis, Genentech). As well, PDT with verteporfin was an uninsured and expensive therapy for this lesion type.
The clinical safety and efficacy of TTT has been demonstrated in a large number of non-randomized clinical papers. As well, subgroup and per-protocol analysis of the recent TTT4CNV randomized clinical trial demonstrates possible clinical benefit in certain subgroups of patients. At the present time, only pegaptanib sodium and ranibizumab have been rigorously proven in randomized clinical trials to show clear benefit for patients with occult membranes. However, these therapies are expensive, require multiple treatments and frequent follow-up, and present risks to the patient resulting from intraocular injections.
Transpupillary thermotherapy may be an alternative therapy for certain cases of exudative AMD, especially in patients unwilling to have intraocular injections or where treatment cost is an issue.
Fareed Ali, MD, FRCS(C), is director of clinical research at the Canadian Centre for Advanced Eye Therapeutics in Toronto, Canada. He has no financial interest in any of the products or therapies mentioned in this article.
|
|
|

|
|
Figure 4. Red-free photo 3 months post-TTT. |
Figure 5. Late-phase fluorescein angiogram 3 months post-TTT. | Figure 6. OCT 3 months post-TTT. |
