







IMPLANTABLE
STEROIDS
A
Viable Alternative to Macular Injections
New
clinical data show two corticosteroid implants for macular disease are safe and
effective.
BY JOHN
M. KING, SENIOR ASSOCIATE EDITOR
From uveitis to diabetic macular edema (DME), sustained release steroid implants are becoming valuable weapons in the retina specialist's armamentarium. Their ability to deliver localized steroid therapy to the eye in implant form is gaining traction as companies discover the benefits of these ocular implants.
Case reports based on clinical data from the sustained drug delivery fluocinolone acetonide intravitreal implant 0.59 mg (Retisert, Bausch & Lomb), were presented at the May 2006 Retinal Physician Symposium. Investigators also presented clinical evidence for treating DME with Posurdex (Allergan Inc.), a biodegradable sustained-release implant that delivers dexamethasone directly to the targeted disease site at the back of the eye.

Retisert is approved by the FDA for the treatment of chronic noninfectious uveitis, affecting the posterior segment of the eye. According to Glenn J. Jaffe, MD, the typical candidate for this implant is a patient who requires periocular, intravitreal or systemic corticosteroids, or who needs immunomodulating agents to control posterior segment inflammation. Frequently, the patient has coexisting iridocyclitis in addition to the posterior uveitis.
"If you have a patient with ocular inflammation who fits this profile, and who also has a coexisting cataract, you may want to consider simultaneous surgery to remove the cataract, place an IOL and implant the Retisert," Dr. Jaffe said. "If a patient has had a vitrectomy and you know the intravitreal injection will be washed out quickly, the fluocinolone implant is also quite efficacious."
Often, a patient's response to a corticosteroid can provide a clue as to how he will respond to a fluocinolone implant. "If a patient previously had a good response to corticosteroids, it's a good sign he will respond well to a fluocinolone implant," Dr. Jaffe said. "Even if he doesn't have an adequate response right away, don't assume he won't respond well to the fluocinolone implant, particularly if the steroids have been delivered either as a periocular injection or as systemic therapy because you may not be getting adequate levels of steroids into the eye. You can achieve higher levels with a fluocinolone implant.
"If an intravitreal corticosteroid injection does not control active posterior uveitis, then a fluocinolone implant is also less likely to be effective," Dr. Jaffe said. "However, in this situation, I would also consider alternative diagnoses, for example, a masquerade syndrome such as large-cell lymphoma."
Dr. Jaffe has a specific procedure for surgery.
AVOID COMPLICATIONS

"Your goal for surgery is to have the implant in the vitreous cavity releasing the drug," Dr. Jaffe said. "A tight wound closure, careful suture management and meticulous conjunctival closure are important to achieve this goal and to avoid complications.
"For local anesthesia, I typically use 4% lidocaine and marcaine
1:1 with hyaluronidase," he continued. "I create a scleral incision approximately
3.5 mm in length and make sure that the pars plana is completely incised. I pass
a double-armed 8-0 prolene suture through the hole in the suture strut and throw
a single tie over the suture strut. Then I take 9/10-full thickness bites on either
side of the scleral incision and close the wound tightly with the anchoring suture,
and use interrupted
9-0 prolene sutures that are tied over the tails on the
anchoring sutures.
"The 9-0 prolene sutures are then rotated to bury the knots, taking care not to rotate the anchoring suture," Dr. Jaffe said. "I use the indirect ophthalmoscope to make sure the implant is properly positioned in the vitreous cavity. The tails on the anchoring suture are trimmed so they will lie flat on the sclera. I then close the conjunctiva with an interrupted suture and give subconjunctival antibiotics. Good conjunctival closure is important because you don't want routes for infection."
The insertion of the implant is just the first step in the procedure, Dr. Jaffe emphasizes.
"When I am counseling a patient, I tell him the implant is potent and should treat his inflammation, which may help reduce the number of medications he will need," Dr. Jaffe said. "But it's important to manage your patient's expectations going in. The first step is the implant surgery. Then you let him know the second step may be a filtering procedure and/or cataract surgery if the surgery hasn't been done beforehand. Although a filtering procedure might not be necessary, if you have certain expectations and communicate them so the patient is in the same frame of mind, you will end up with a happy patient."
|
|
|
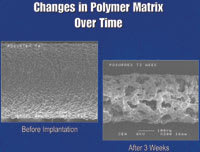
Posurdex is a biodegradable dexamethasone implant in which the drug is incorporated into the polymer matrix. The implant is a sustained medication release device, and while the drug is released, the polymer begins to erode away. |
POSURDEX FOR DME
Steroids have a history of demonstrated efficacy in treating DME. The multifactorial effect of steroids in dealing with leukocyte endothelial cell adhesion, tight junction protein remodeling, and inflammatory mediators makes steroids a very appealing part of DME treatment. Going forward, one challenge will be the use of steroids vs. anti-VEGF compounds that are coming onto the market. According to one retinal specialist, this is an area in which further research is needed.
"Triamcinolone acetonide (Kenalog) has been the drug we've used for diseases associated with retinal vascular permeability because of its availability," said Baruch D. Kuppermann, MD, PhD. "But we know it is not formulated for the eye. There has been a history of sterile endophthalmitis associated with this formulation, and more recently, there have been reports of retinal cell toxicity associated with its use. Other steroids appear more ideal from a potency standpoint. For example, dexamethasone and betamethasone have more anti-inflammatory potency than triamcinolone."
Dr. Kuppermann and colleagues looked at the effect of a variety of commonly available steroids on retinal cells in culture in their laboratory with the goal of determining if there are differences in their retinal cell toxicity.
DOSING FACTORS AND TOXICITY
"First, we tried triamcinolone," Dr Kuppermann said. "Even at relatively low doses, we noted significant toxicity to both retinal pigment epithelial and neurosensory cells in culture. Surprisingly, the supernatant vehicle did not show toxicity. Furthermore, a preservative-free formulation of triamcinolone was also toxic to the retinal cells in culture, suggesting a direct toxic effect of the drug and not the vehicle." Dr. Kuppermann's group found similar results in many of the other steroids they studied.
"However, when we tested dexamethasone, which is the most potent of all the steroids, we saw no signs of toxicity until we used a dose 10 times what we use clinically in an injection of free dexamethasone for a case of endophthalmitis, for example," Dr. Kuppermann said. "Dexamethasone was the most potent and yet the least toxic steroid in the assays we used on our retinal pigment epithelial and neurosensory cell lines in culture." Furthermore, the drug levels associated with the sustained-release Posurdex implant are well below drug levels associated with free injection of the dissolved drug, according to Dr. Kuppermann. "This raises the possibility that dexamethasone may be a viable alternative to triamcinolone, due to its potency and minimal retinal toxicity," he said.
One caveat associated with dexamethasone is its short half-life. "For dexamethasone to have significant clinical utility, it is likely that we will need to use it in a drug delivery system," Dr. Kuppermann said. "With the Posurdex implant, we have such a system: a biodegradable dexamethasone implant in which the drug is incorporated into the polymer matrix. The Posurdex implant is a sustained medication release device and while the drug is released, the polymer begins to erode away. More drug release brings more polymer erosion until the entire drug is released. Then the residual polymer that is left breaks down inside the eye."
According to Dr. Kuppermann, a newer sutureless injectable Posurdex implant can be inserted into the eye in an office setting. Clinical data also show the new version of the Posurdex implant is better than or equal to the older incisional placement in terms of safety and efficacy because there is no vitreous hemorrhage, and there may be less effect on intraocular pressure.
"The overall conclusion is that in patients with persistent, refractory macular edema, the 700-microgram dexamethasone DDS Posurdex implant, produces statistically and clinically significant improvements in visual acuity," he said. "Phase 3 clinical trials are now under way to assess the efficacy of Posurdex for treating DME and macular edema secondary to vein occlusion. Other trials examining the role of Posurdex in the treatment of uveitis and age-related macular degeneration are also being considered."