







Imaging
Between AMPPE and Serpiginous Choroidopathy
ampiginous chorioretinitis in a 16-year-old male
A 16-year-old white male presented with a blind spot in his central vision OS for 5 weeks. Ocular history was notable for strabismus as a child. Past medical history was significant for thyroid disease treated with thyroid replacement hormone and growth hormone.
On initial exam VA was 20/20 OD and 20/150 OS. Anterior segment exam was normal. Retinal exam was significant for a flat hypo- and hyperpigmented scar in the posterior pole OD. The left eye had a similar lesion, but with discrete creamy white lesions off the inferior arcade (Figure 1A).
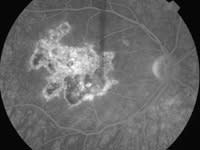
Fluorescein angiography revealed window defects with staining of the scarred regions of both eyes. The inferior lesion on the left eye revealed blocking in the early stages of the angiogram with late hyperfluorescence (Figures 1B, 1C). Patient was diagnosed with acute posterior multifocal placoid pigment epitheliopathy (AMPPE) and observed. Patient's vision improved to 20/40, and the retina exam remained stable.
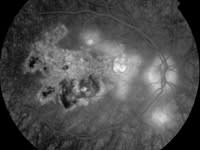
One year after initial presentation, patient presented with new blind spot in the right eye. Macular exam was significant for at least 3 new areas of inflammatory foci superonasal to the fovea and inferior to the optic disc (Figures 2A, 2B, 2C).
Patient had an initial diagnosis of AMPPE. The initial fluorescein was consistent with this diagnosis, showing areas of early blockage with late hyperflourescence.1 However, recurrence of AMPPE-like lesions is distinctly unusual, but more frequently seen with serpiginous choridopathy, which also has a similar fluorescein pattern.2 In addition, the new configuration of the lesions emanating from the optic nerve is suggestive of serpiginous.
There is a continuum between AMPPE and serpiginous choroidopathy called ampiginous chorioretinitis (relentless placoid chorioretinitis) which combines features of both syndromes.3
-- Darcy H. Wolsey, MD, MPH, Moran Eye Center, Salt Lake City, Utah

|

|
|

|

|
|
|
|
|
| Figure 1A. On initial examination, lesion with several discrete creamy white lesions off the inferior arcade OS. Figures 1B, 1C. On initial examination, FA revealed an inferior lesion OS, blocking in the early stages of the angiogram, and late hyperfluorescence. |
Figures 2A, 2B, 2C. 1 year after initial presentation, the macular exam was significant for at least 3 new areas of inflammatory foci superonasal to the fovea and inferior to the optic disc OD. | |
|
IMAGES: PAULA MORRIS, CRA, MORAN EYE CENTER, UNIVERSITY OF UTAH, SALT LAKE CITY |
||
REFERENCES
1. Roberts TV, Mitchell P. Acute posterior multifocal placoid pigment epitheliopathy: A long term study. Australian and New Zealand Journal of Ophthalmology. 1997;25: 277-281.
2. Schatz H, McDonald HR, Johnson RN, Everett A. Geographic helicoid peripapillary choroidopathy (serpiginous choroiditis). Retina Third Edition. Editor Schachat AP. Mosby, St. Louis. 2001;1746-1755.
3. Jones BE, Jampol LM, Yannuzzi LA, Tittl M, et al. Relentless placoid chorioretinitis. A new entity or an unusual variant of serpiginous chorioretinitis? Arch Ophthalmol. 2000;118:931-938.